

The Role of Incretins on Insulin Function and Glucose Homeostasis
- PMID: 33782700
- PMCID: PMC8168943
- DOI: 10.1210/endocr/bqab065
The Role of Incretins on Insulin Function and Glucose Homeostasis
Abstract
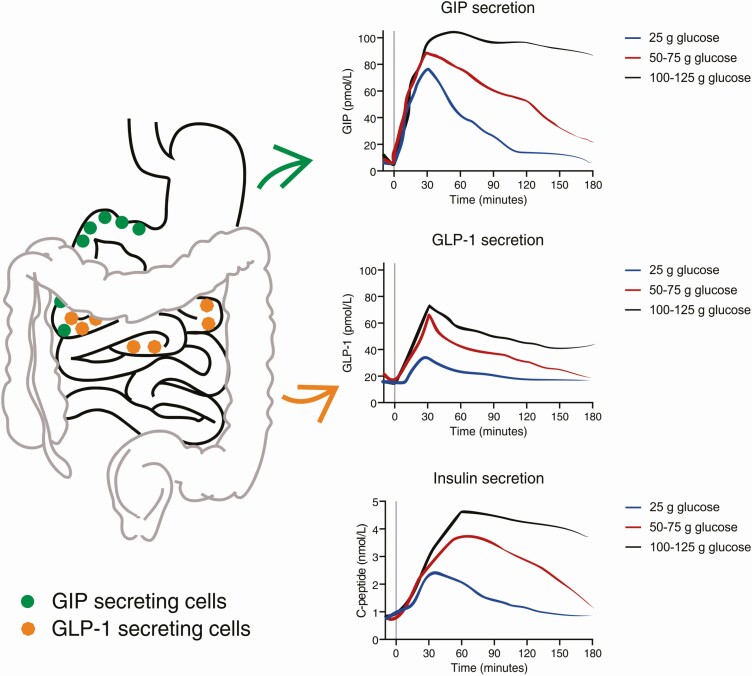
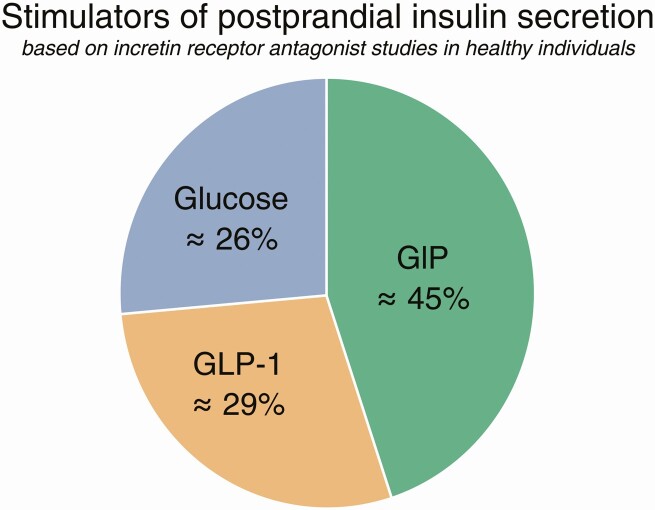
The incretin effect-the amplification of insulin secretion after oral vs intravenous administration of glucose as a mean to improve glucose tolerance-was suspected even before insulin was discovered, and today we know that the effect is due to the secretion of 2 insulinotropic peptides, glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1). But how important is it? Physiological experiments have shown that, because of the incretin effect, we can ingest increasing amounts of amounts of glucose (carbohydrates) without increasing postprandial glucose excursions, which otherwise might have severe consequences. The mechanism behind this is incretin-stimulated insulin secretion. The availability of antagonists for GLP-1 and most recently also for GIP has made it possible to directly estimate the individual contributions to postprandial insulin secretion of a) glucose itself: 26%; b) GIP: 45%; and c) GLP-1: 29%. Thus, in healthy individuals, GIP is the champion. When the action of both incretins is prevented, glucose tolerance is pathologically impaired. Thus, after 100 years of research, we now know that insulinotropic hormones from the gut are indispensable for normal glucose tolerance. The loss of the incretin effect in type 2 diabetes, therefore, contributes greatly to the impaired postprandial glucose control.
Keywords: exendin 9-39; glucagon-like peptide-1 (GLP-1); glucose-dependent insulinotropic polypeptide (GIP); hormone antagonists; hormone coagonists.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- Mering Jv, Minkowski O. Diabetes mellitus nach Pankreasexstirpation. Archiv f experiment Pathol u Pharmakol. 1890; 26: 371-387.
-
- von Mering J, Minkowski O. Diabetes mellitus and pancreas extirpation. Arch Exp Path Pharmak. 1889;21:371-390.
-
- Zunz E, La Barre J. Contributions a l’étude des variation physiologiques de la sécrétion interne de pancréas: relations entre les secretions externe et interne du pancréas. Archs Int Physiol Biochim. 1929;31(1):20-44.
-
- McIntyre N, Holdsworth CD, Turner DS. New interpretation of oral glucose tolerance. Lancet. 1964;2(7349):20-21. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
