

Strategies for successful implementation of resuscitative endovascular balloon occlusion of the aorta in an urban Level I trauma center
- PMID: 33783417
- PMCID: PMC8375411
- DOI: 10.1097/TA.0000000000003198
Strategies for successful implementation of resuscitative endovascular balloon occlusion of the aorta in an urban Level I trauma center
Abstract
Background: The rationale for resuscitative endovascular balloon occlusion of the aorta (REBOA) is to control life-threatening subdiaphragmatic bleeding and facilitate resuscitation; however, incorporating this into the resuscitative practices of a trauma service remains challenging. The objective of this study is to describe the process of successful implementation of REBOA use in an academic urban Level I trauma center. All REBOA procedures from April 2014 through December 2019 were evaluated; REBOA was implemented after surgical faculty attended a required and internally developed Advanced Endovascular Strategies for Trauma Surgeons course. Success was defined by sustained early adoption rates.
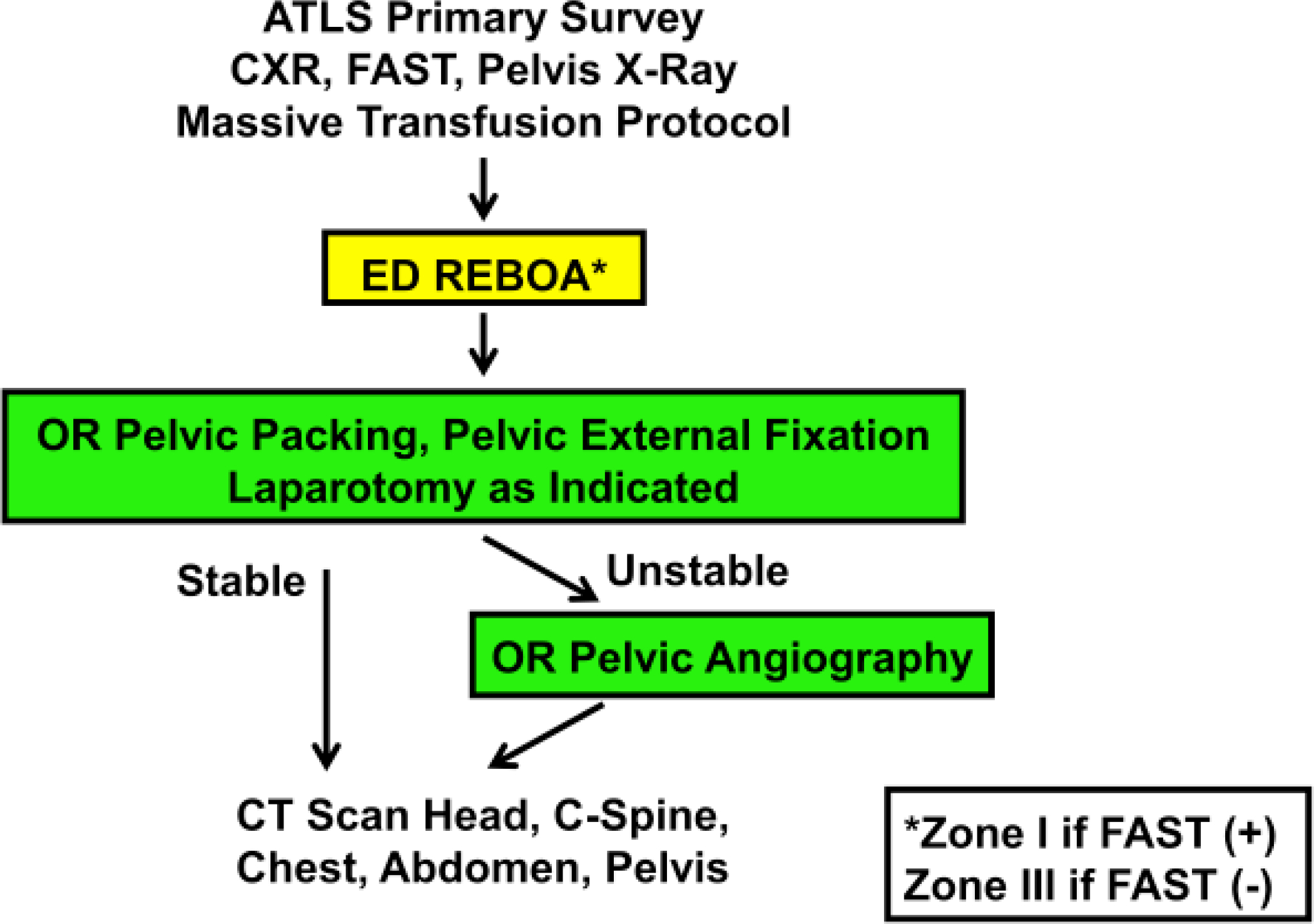
Methods: An institutional protocol was published, and a REBOA supply cart was placed in the emergency department with posters attached to depict technical and procedural details. A focused professional practice evaluation was utilized for the first three REBOA procedures performed by each faculty member, leading to internal privileging.
Results: Resuscitative endovascular balloon occlusion of the aorta was performed in 97 patients by nine trauma surgeons, which is 1% of the total trauma admissions during this time. Each surgeon performed a median of 12 REBOAs (interquartile range, 5-14). Blunt (77/97, 81%) or penetrating abdominopelvic injuries (15/97, 15%) comprised the main injury mechanisms; 4% were placed for other reasons (4/97), including ruptured abdominal aortic aneurysms (n = 3) and preoperatively for a surgical oncologic resection (n = 1). Overall survival was 65% (63/97) with a steady early adoption trend that resulted in participation in a Department of Defense multicenter trial.
Conclusion: Strategies for how departments adopt new procedures require clinical guidelines, a training program focused on competence, and a hospital education and privileging process for those acquiring new skills.
Level of evidence: Therapeutic, level V.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Figures



References
-
- Davidson AJ, Russo RM, Reva VA, Brenner ML, Moore LJ, Ball C, Bulgar E, Fox CJ, DuBose JJ, Moore EE, et al., The pitfalls of resuscitative endovascular balloon occlusion of the aorta: Risk factors and mitigation strategies. J Trauma Acute Care Surg. 2018. 84(1): p. 192–202. - PubMed
-
- DuBose JJ, Scalea TM, Brenner M, Skiada D, Inaba K, Cannon J, Moore L, Holcomb J, Turay D, Arbabi CN, et al., The AAST prospective Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery (AORTA) registry: Data on contemporary utilization and outcomes of aortic occlusion and resuscitative balloon occlusion of the aorta (REBOA). J Trauma Acute Care Surg. 2016. 81(3): p. 409–19. - PubMed
-
- Glaser JJ, Czerwinski A, Alley A, Keyes M, Piacentino V, and Pepe A, Implementing a REBOA program outside of the ivory tower: initial case series and lessons learned at a community trauma center. JEVTM. 2018. 2(3).
-
- Biffl WL, Fox CJ, and Moore EE, The role of REBOA in the control of exsanguinating torso hemorrhage. J Trauma Acute Care Surg, 2015. 78(5): p. 1054–8. - PubMed
-
- Villamaria CY, Eliason JL, Napolitano LM, Stansfield RB, Spencer JR, and Rasmussen TE, Endovascular Skills for Trauma and Resuscitative Surgery (ESTARS) course: curriculum development, content validation, and program assessment. J Trauma Acute Care Surg. 2014. 76(4): p. 929–35; discussion 935–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
