

A phase I study of anti-BCMA CAR T cell therapy in relapsed/refractory multiple myeloma and plasma cell leukemia
- PMID: 33784005
- PMCID: PMC7943908
- DOI: 10.1002/ctm2.346
A phase I study of anti-BCMA CAR T cell therapy in relapsed/refractory multiple myeloma and plasma cell leukemia
Abstract
Background: Relapsed/refractory (R/R) multiple myeloma (MM) patients and primary plasma cell leukemia (PCL) have an unfavorable prognosis and no effective treatment. This study was designed to assess the safety and preliminary efficacy of a novel anti-B-cell maturation antigen (BCMA) chimeric antigen receptor (CAR) T cell in R/R MM and PCL.
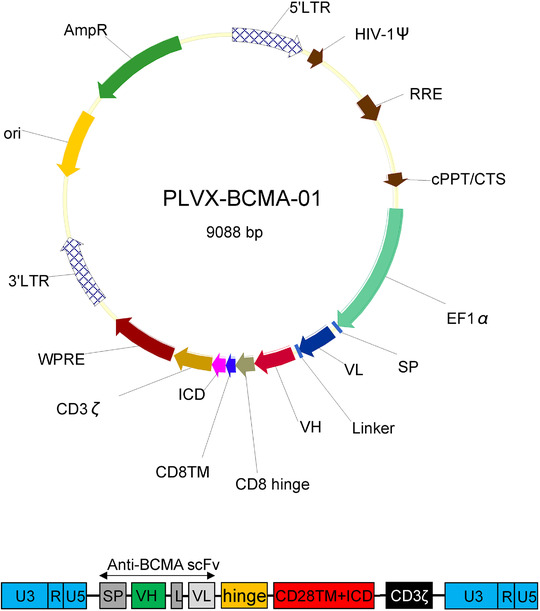
Methods: Between February 22, 2017, and June 25, 2018, 28 R/R and two R/R primary PCL patients received a median dose of 11.2 × 106 CAR+ cells/kg. The subjects were refractory to a proteasome inhibitor and/or an immunomodulatory agent. Fludarabine and cyclophosphamide were given as lymphodepletion chemotherapy.
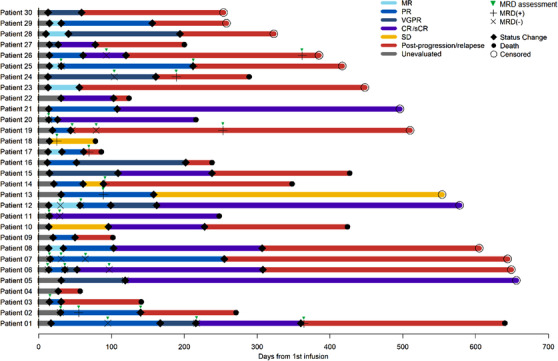
Results: Results for these 30 consecutive patients who received an anti-BCMA CAR T cell infusion are reported. The patients had received a median of four prior lines of therapy. A total of 44 different types of adverse events were recorded, and hematologic toxic effects were the most common events of any grade during treatment. Hematologic toxic effects were also the most common events of grade 3 or higher. A total of 29 patients (96.7%) had cytokine release syndrome, which was of grade 1 or 2 in 24 patients (80%) and grade 3 in five patients (16.7%). Neurologic toxic effects only occurred in one patient (3.3%) and were of grade 1. The objective response rate was 90%, and the complete response rate was 43.3%. With a median follow-up of 12.6 months, the median progression-free survival (PFS) and overall survival were 5.2 months and 14.0 months. One of the two primary PCL achieved a complete response with a PFS of 307 days. The other patients achieved a very good partial response with a PFS of 117 days.
Conclusions: Anti-BCMA CAR T cell treatment is safe and highly active in R/R multiple myeloma.
Keywords: anti-BCMA CAR T cell; multiple myeloma; plasma cell leukemia; relapsed/refractory.
© 2021 The Authors. Clinical and Translational Medicine published by John Wiley & Sons Australia, Ltd on behalf of Shanghai Institute of Clinical Bioinformatics.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures




References
-
- Laubach JP, Voorhees PM, Hassoun H, Jakubowiak A, Lonial S, Richardson PG. Current strategies for treatment of relapsed/refractory multiple myeloma. Expert Rev Hematol. 2014;7(1):97–111. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials