

Effect of Intravitreous Anti-Vascular Endothelial Growth Factor vs Sham Treatment for Prevention of Vision-Threatening Complications of Diabetic Retinopathy: The Protocol W Randomized Clinical Trial
- PMID: 33784735
- PMCID: PMC8010644
- DOI: 10.1001/jamaophthalmol.2021.0606
Effect of Intravitreous Anti-Vascular Endothelial Growth Factor vs Sham Treatment for Prevention of Vision-Threatening Complications of Diabetic Retinopathy: The Protocol W Randomized Clinical Trial
Abstract
Importance: The role of anti-vascular endothelial growth factor injections for the management of nonproliferative diabetic retinopathy (NPDR) without center-involved diabetic macular edema (CI-DME) has not been clearly established.
Objective: To determine the efficacy of intravitreous aflibercept injections compared with sham treatment in preventing potentially vision-threatening complications in eyes with moderate to severe NPDR.
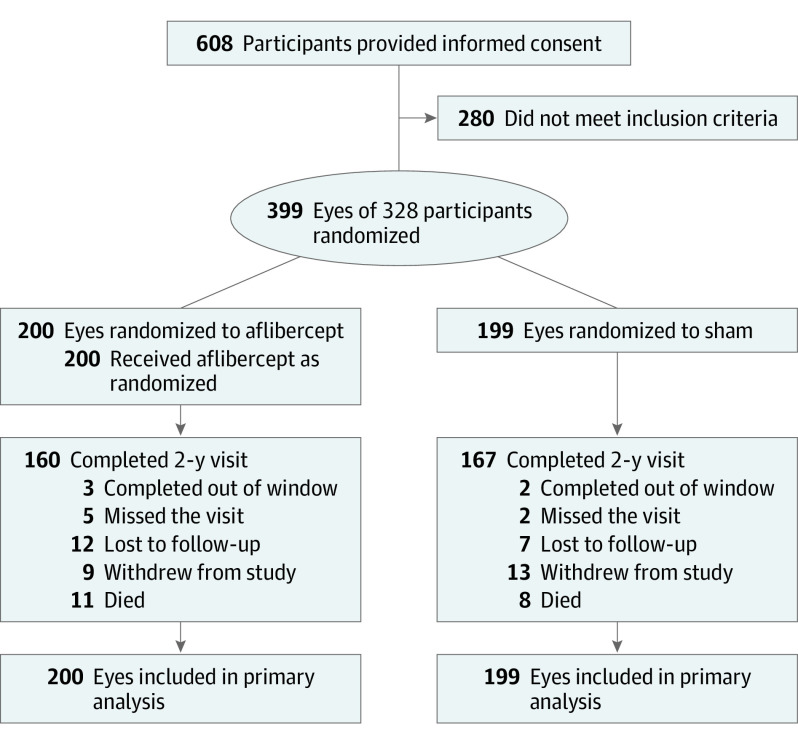
Design, setting, and participants: Data for this study were collected between January 15, 2016, and May 28, 2020, from the ongoing DRCR Retina Network Protocol W randomized clinical trial, conducted at 64 US and Canadian sites among 328 adults (399 eyes) with moderate to severe NPDR (Early Treatment Diabetic Retinopathy Study severity level, 43-53), without CI-DME. Analyses followed the intent-to-treat principle.
Interventions: Eyes were randomly assigned to 2.0 mg of aflibercept injections (n = 200) or sham (n = 199) given at baseline; 1, 2, and 4 months; and every 4 months through 2 years. Between 2 and 4 years, treatment was deferred if the eye had mild NPDR or better. Aflibercept was administered in both groups if CI-DME with vision loss (≥10 letters at 1 visit or 5-9 letters at 2 consecutive visits) or high-risk proliferative diabetic retinopathy (PDR) developed.
Main outcomes and measures: Development of CI-DME with vision loss or PDR through May 2020, when the last 2-year visit was completed.
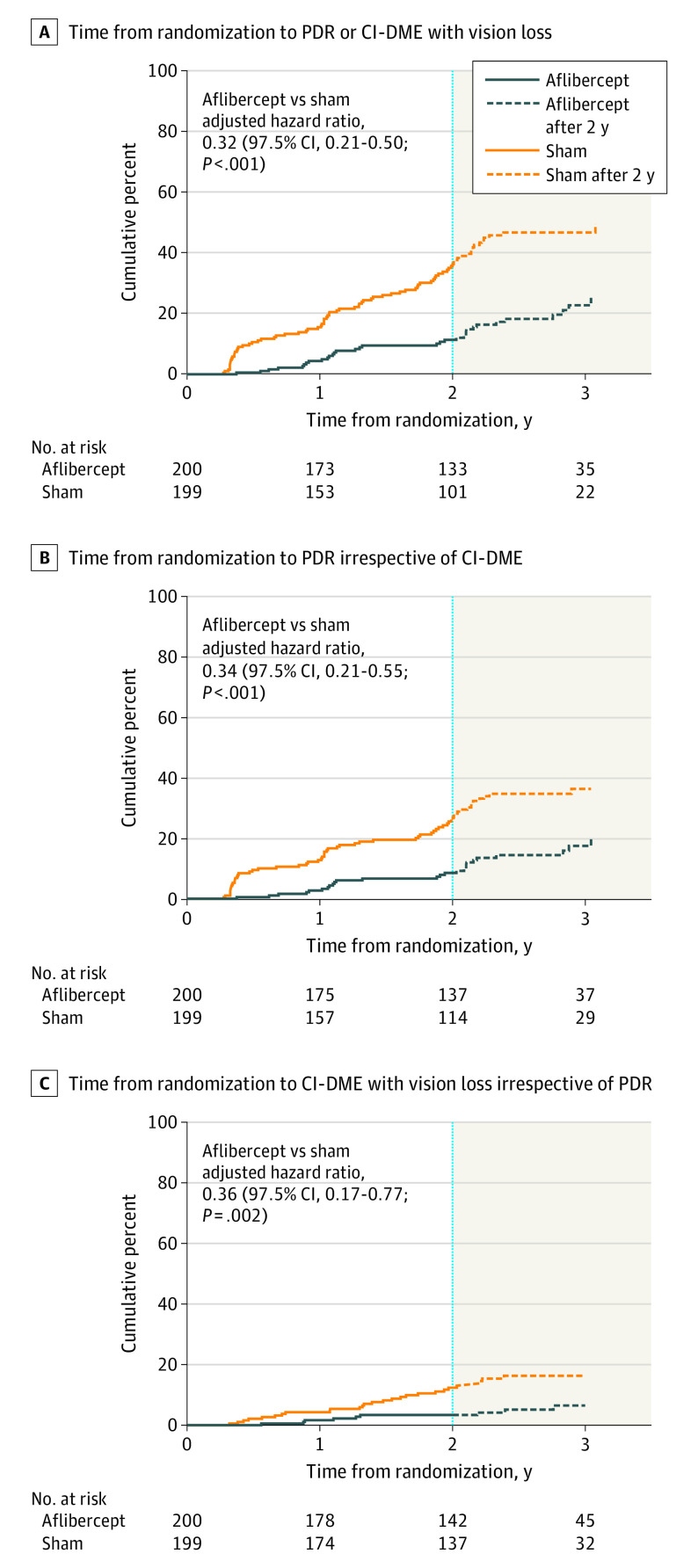
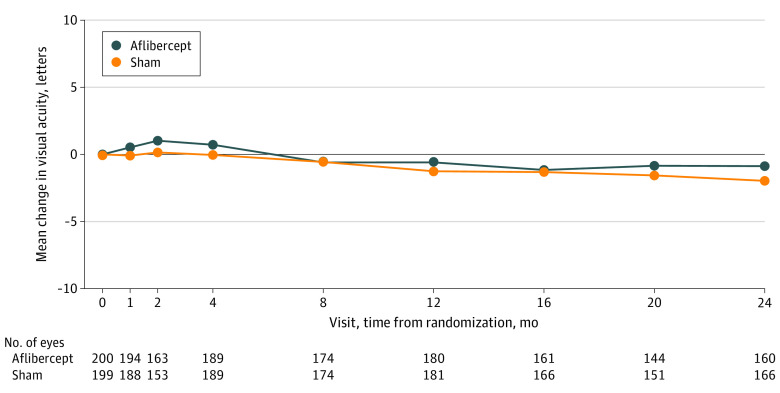
Results: Among the 328 participants (57.6% men [230 of 399 eyes]; mean [SD] age, 56 [11] years), the 2-year cumulative probability of developing CI-DME with vision loss or PDR was 16.3% with aflibercept vs 43.5% with sham. The overall hazard ratio for either outcome was 0.32 (97.5% CI, 0.21-0.50; P < .001), favoring aflibercept. The 2-year cumulative probability of developing PDR was 13.5% in the aflibercept group vs 33.2% in the sham group, and the 2-year cumulative probability of developing CI-DME with vision loss was 4.1% in the aflibercept group vs 14.8% in the sham group. The mean (SD) change in visual acuity from baseline to 2 years was -0.9 (5.8) letters with aflibercept and -2.0 (6.1) letters with sham (adjusted mean difference, 0.5 letters [97.5% CI, -1.0 to 1.9 letters]; P = .47).
Conclusions and relevance: In this randomized clinical trial, among eyes with moderate to severe NPDR, the proportion of eyes that developed PDR or vision-reducing CI-DME was lower with periodic aflibercept compared with sham treatment. However, through 2 years, preventive treatment did not confer visual acuity benefit compared with observation plus treatment with aflibercept only after development of PDR or vision-reducing CI-DME. The 4-year results will be important to assess longer-term visual acuity outcomes.
Trial registration: ClinicalTrials.gov Identifier: NCT02634333.
Conflict of interest statement
Figures
Comment in
-
Prevention of Severe Nonproliferative Diabetic Retinopathy Progression With More at Stake Than Visual Acuity.JAMA Ophthalmol. 2021 Jul 1;139(7):714-716. doi: 10.1001/jamaophthalmol.2021.0625. JAMA Ophthalmol. 2021. PMID: 33784733 No abstract available.
-
Practicality of Prophylactic Aflibercept to Reduce Diabetic Retinopathy Progression.JAMA Ophthalmol. 2021 Jul 1;139(7):713-714. doi: 10.1001/jamaophthalmol.2021.0624. JAMA Ophthalmol. 2021. PMID: 33784736 No abstract available.
References
-
- Gross JG, Glassman AR, Jampol LM, et al. ; Writing Committee for the Diabetic Retinopathy Clinical Research Network . Panretinal photocoagulation vs intravitreous ranibizumab for proliferative diabetic retinopathy: a randomized clinical trial. JAMA. 2015;314(20):2137-2146. doi: 10.1001/jama.2015.15217 - DOI - PMC - PubMed
-
- Sivaprasad S, Prevost AT, Vasconcelos JC, et al. ; CLARITY Study Group . Clinical efficacy of intravitreal aflibercept versus panretinal photocoagulation for best corrected visual acuity in patients with proliferative diabetic retinopathy at 52 weeks (CLARITY): a multicentre, single-blinded, randomised, controlled, phase 2b, non-inferiority trial. Lancet. 2017;389(10085):2193-2203. doi: 10.1016/S0140-6736(17)31193-5 - DOI - PubMed
-
- Wilkinson CP, Ferris FL 3rd, Klein RE, et al. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology. 2003;110(9):1677-1682. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
