

Isolated intestinal Ganglioneuromatosis: case report and literature review
- PMID: 33785023
- PMCID: PMC8008650
- DOI: 10.1186/s13052-021-01024-5
Isolated intestinal Ganglioneuromatosis: case report and literature review
Abstract
Background: Intestinal Ganglioneuromatosis (IG) is a rare disorder of the enteric nervous system. In pediatric age it is often associated with genetic syndromes such as Neurofibromatosis 1 (NF1), multiple endocrine neoplasia type 2B (MEN2B) and Cowden syndrome (PTEN mutation), and ganglioneuromas (GNs) may be sometimes the first sign of the disease. Isolated GNs are rare and sporadic. Clinical symptom vary and depend on the size and on the location of the GNs. This disorder affects intestinal motility and it, consequently, causes changes in bowel habits, abdominal pain, occlusive symptoms and rarely lower gastrointestinal bleeding secondary to ulceration of the intestinal mucosa. On the other hand, patients can remain asymptomatic for many years.
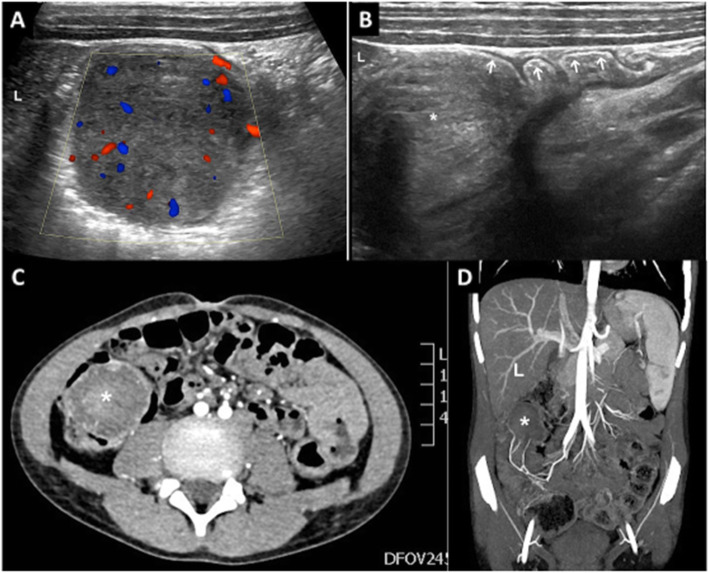
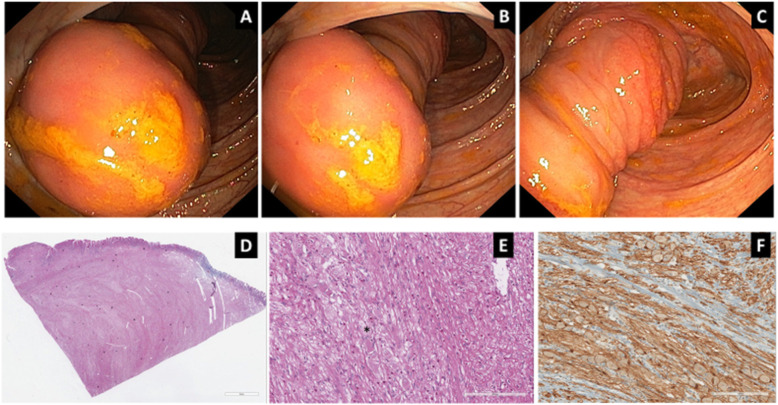
Case presentation: We describe a 9-year-old boy referred to our emergency department for right lower quadrant abdominal pain. No familial history for gastrointestinal disorders. No history of fever or weight loss. At physical examination, he had diffused abdominal pain. Abdominal ultrasonography showed a hypoechoic formation measuring 41.8 mm by 35 mm in the right lower quadrant of the abdomen. Routine blood tests were normal, but fecal occult blood test was positive. Abdominal TC confirmed the hypodense formation, of about 5 cm in transverse diameter, in the right hypochondrium that apparently invaginated in the caecum-last ileal loop. Colonoscopy showed in the cecum an invaginated polypoid lesion of the terminal ileal loop. Laparoscopic resection of the polypoid lesion was performed. Histological diagnosis of the large neoplasm observed in the terminal ileum was diffuse ganglioneuromatosis. NF1, RET and PTEN gene tests resulted negative for specific mutations. At the 1 year follow-up, the patient presented good general condition and blood tests, fecal occult blood test, esophagogastroduodenoscopy, colonoscopy and MR-enterography were negative.
Conclusions: Only few cases are reported in literature of IG in pediatric age. Although rare, the present case suggests that this disorder must be taken in consideration in every patient with GI symptoms such as abdominal pain, constipation, lower intestinal bleeding, in order to avoid a delayed diagnosis.
Keywords: Abdominal pain; Case report; Intestinal ganglioneuromatosis; Pediatric; Polyps.
Conflict of interest statement
No competing interests for all authors.
Figures
References
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
