

Harmine is an effective therapeutic small molecule for the treatment of cardiac hypertrophy
- PMID: 33785860
- PMCID: PMC8724320
- DOI: 10.1038/s41401-021-00639-y
Harmine is an effective therapeutic small molecule for the treatment of cardiac hypertrophy
Abstract
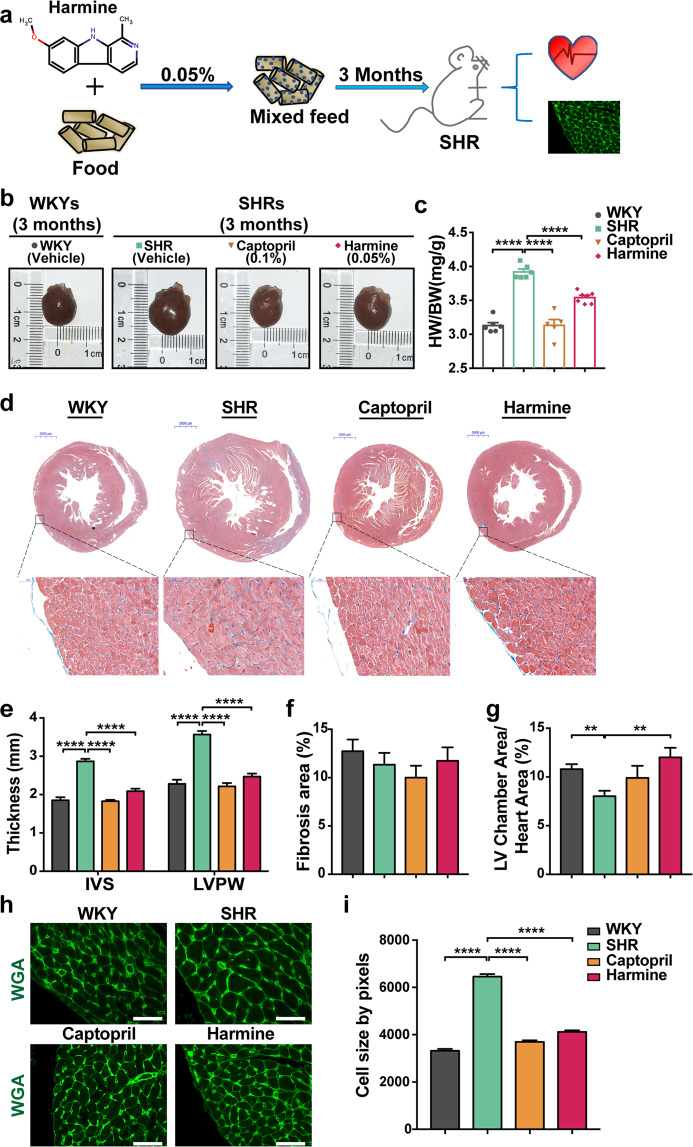
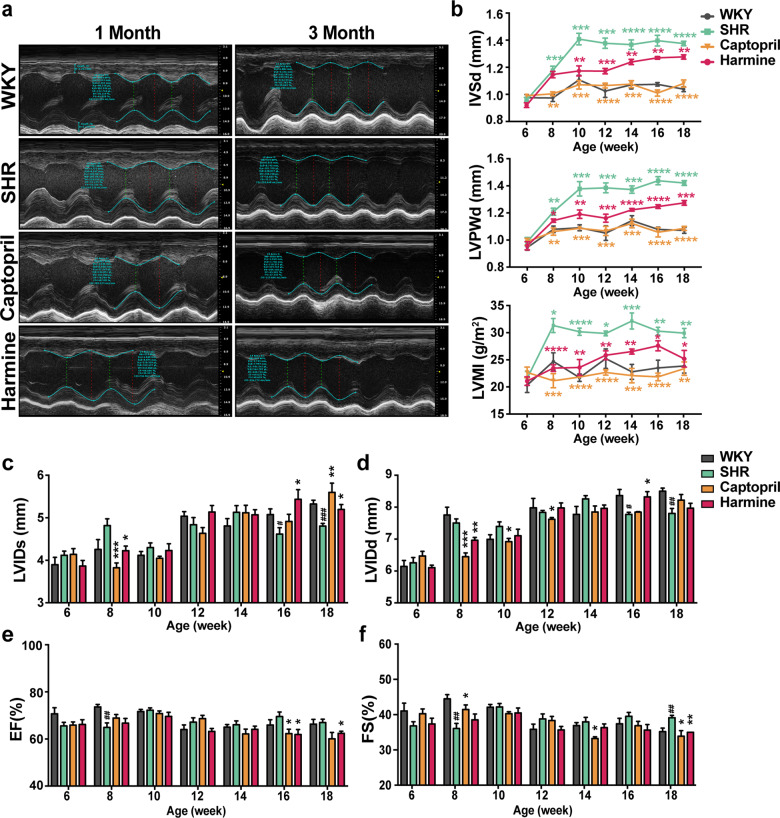
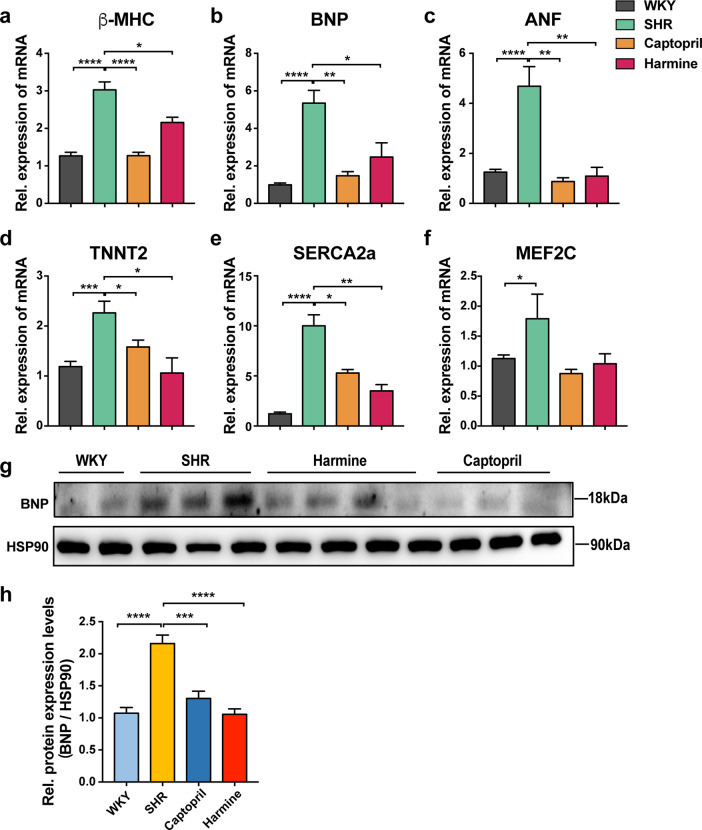
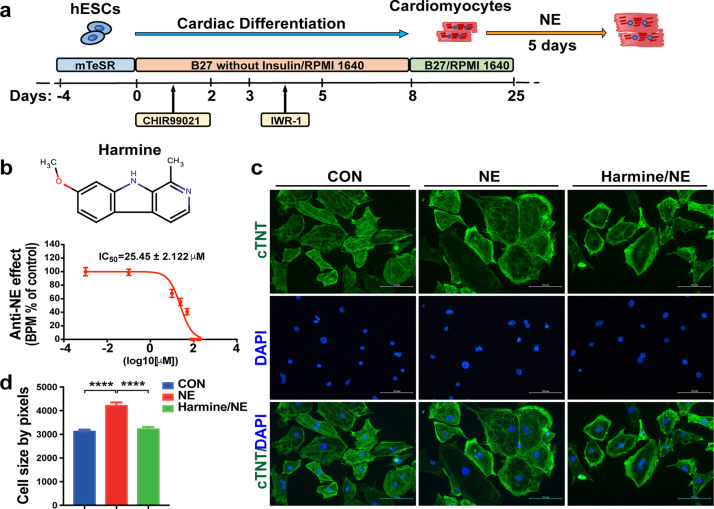
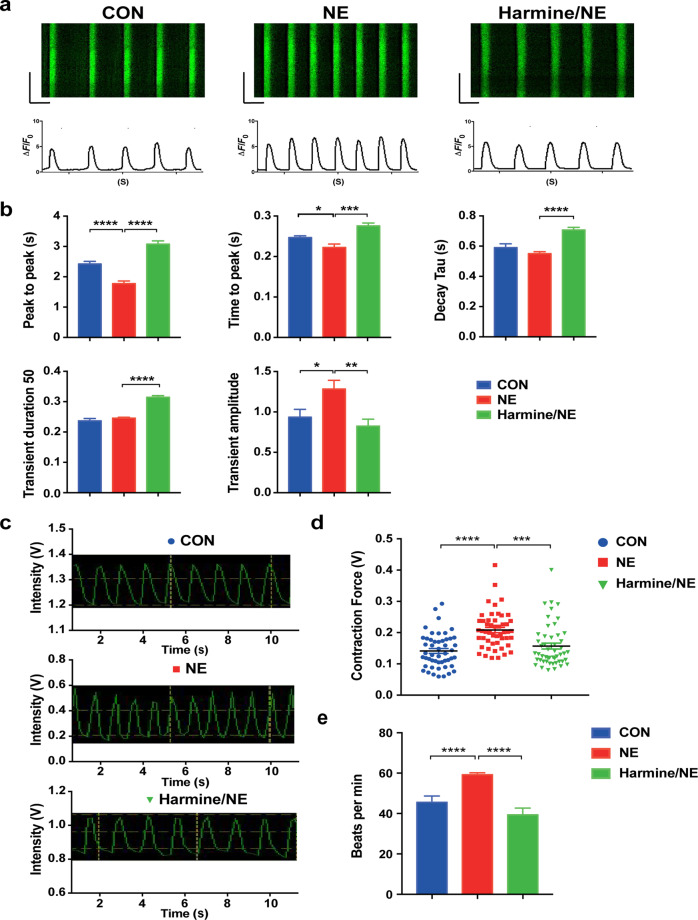
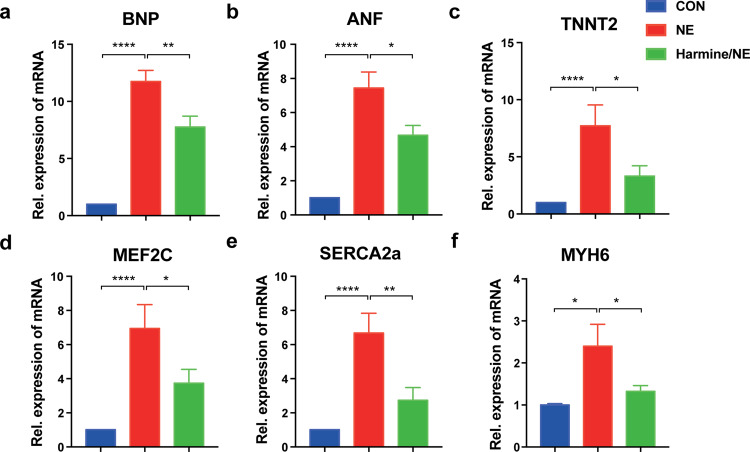
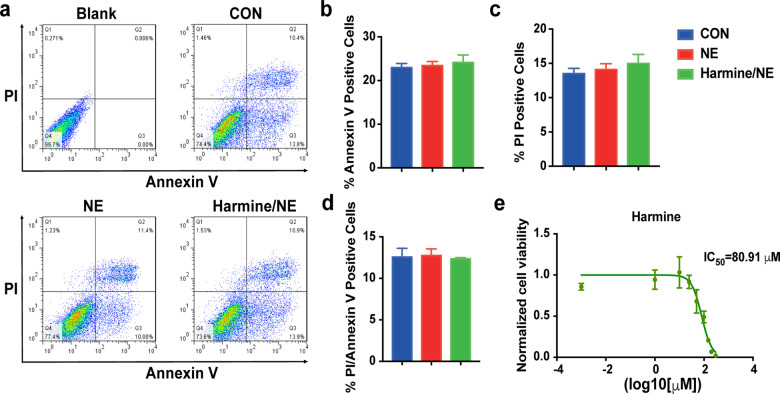
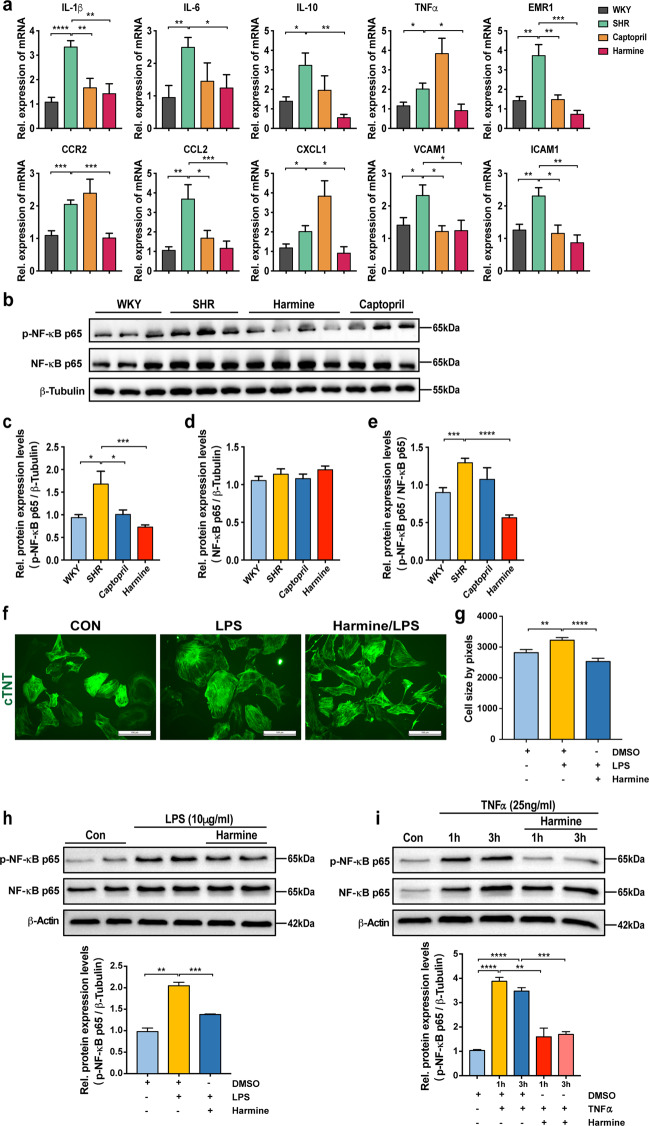
Harmine is a β-carboline alkaloid isolated from Banisteria caapi and Peganum harmala L with various pharmacological activities, including antioxidant, anti-inflammatory, antitumor, anti-depressant, and anti-leishmanial capabilities. Nevertheless, the pharmacological effect of harmine on cardiomyocytes and heart muscle has not been reported. Here we found a protective effect of harmine on cardiac hypertrophy in spontaneously hypertensive rats in vivo. Further, harmine could inhibit the phenotypes of norepinephrine-induced hypertrophy in human embryonic stem cell-derived cardiomyocytes in vitro. It reduced the enlarged cell surface area, reversed the increased calcium handling and contractility, and downregulated expression of hypertrophy-related genes in norepinephrine-induced hypertrophy of human cardiomyocytes derived from embryonic stem cells. We further showed that one of the potential underlying mechanism by which harmine alleviates cardiac hypertrophy relied on inhibition of NF-κB phosphorylation and the stimulated inflammatory cytokines in pathological ventricular remodeling. Our data suggest that harmine is a promising therapeutic agent for cardiac hypertrophy independent of blood pressure modulation and could be a promising addition of current medications for cardiac hypertrophy.
Keywords: NE; SHR; cardiac hypertrophy; hESCs-derived cardiomyocytes; harmine; inflammatory.
© 2021. The Author(s), under exclusive licence to CPS and SIMM.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Hill JA, Olson EN. Cardiac plasticity. N Engl J Med. 2008;358:1370–80. - PubMed
-
- Frey N, Katus HA, Olson EN, Hill JA. Hypertrophy of the heart: a new therapeutic target? Circulation. 2004;109:1580–9. - PubMed
-
- Berenji K, Drazner MH, Rothermel BA, Hill JA. Does load-induced ventricular hypertrophy progress to systolic heart failure? Am J Physiol Heart Circ Physiol. 2005;289:H8–h16. - PubMed
-
- Lorell BH, Carabello BA. Left ventricular hypertrophy: pathogenesis, detection, and prognosis. Circulation. 2000;102:470–9. - PubMed
-
- Maron BJ, Maron MS. Hypertrophic cardiomyopathy. Lancet. 2013;381:242–55. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
