

Postoperative pain control with continuous paravertebral nerve block and intercostal nerve block after two-port video-assisted thoracic surgery
- PMID: 33786144
- PMCID: PMC7991946
- DOI: 10.5114/wiitm.2020.99349
Postoperative pain control with continuous paravertebral nerve block and intercostal nerve block after two-port video-assisted thoracic surgery
Abstract
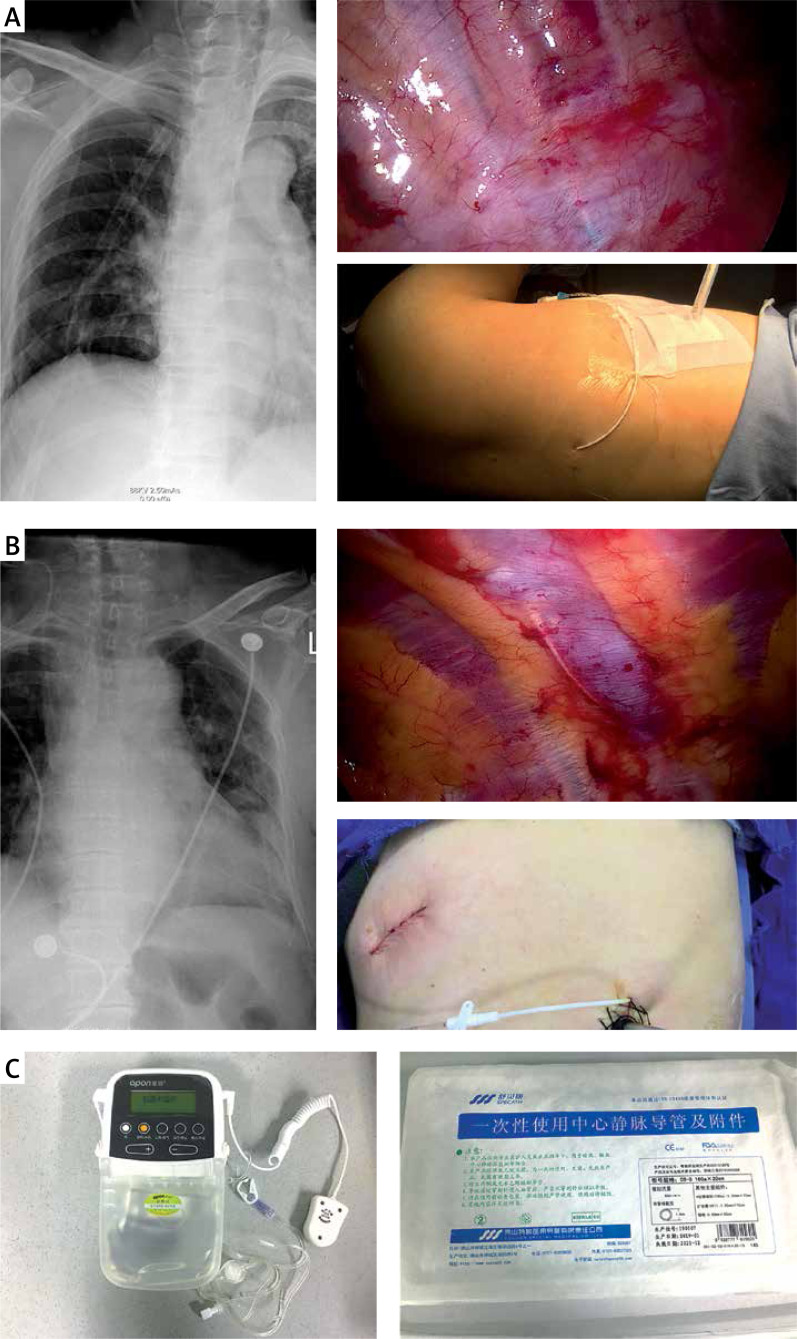
Introduction: Effective pain control after video-assisted thoracic surgery (VATS) is critical because of the correlation between postoperative pain and recovery after surgery. Due to the limitations of traditional analgesic modalities, in this study, we present a method of placing a paravertebral catheter (PVC) or an intercostal catheter (ICC) in the sub-pleural space, followed by continuous ropivacaine injection by an infusion pump after surgery.
Aim: To investigate the impact of continuous paravertebral nerve block and intercostal nerve block on postoperative pain control in patients who underwent two-port thoracic surgery.
Material and methods: A total of 269 patients underwent various types of two-port VATS at Hwa Mei Hospital. Among them, we retrospectively compared paravertebral block versus intercostal nerve block to intravenous patient-controlled analgesia after VATS. Data regarding postoperative pain score on postoperative day 0, 1, 2, 3, and discharge day pain score, tramadol requirements, drainage duration, postoperative hospital stay, postoperative complications, and chronic pain 3 months after surgery were collected and analyzed.
Results: Compared with the control group, patients who received a continuous nerve block, including the PVC group and ICC group, had a lower postoperative pain score (p < 0.001), shorter drainage duration (4.63 ±2.84 to 5.61 ±2.66 days, p = 0.004), reduced postoperative hospital stay (6.04 ±3.01 to 7.69 ±3.26 days, p < 0.001), and a reduced frequency of tramadol (0.95 ±1.27 1.79 ±2.13 times, p < 0.001). Additionally, there was no significant difference in chronic pain between groups.
Conclusions: In our study, PVC and ICC appeared to be safe and effective analgesic techniques to reduce postoperative pain, thus shortening the duration of postoperative hospital stay and improving the satisfaction of patients.
Keywords: Enhanced Recovery After Surgery program; intercostal nerve block; minimally invasive surgery; paravertebral nerve block; postoperative analgesia; video-assisted thoracic surgery.
Copyright: © 2020 Fundacja Videochirurgii.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


Similar articles
-
Management of post-operative pain by placement of an intraoperative intercostal catheter after single port video-assisted thoracoscopic surgery: a propensity-score matched study.J Thorac Dis. 2016 Jun;8(6):1087-93. doi: 10.21037/jtd.2016.04.01. J Thorac Dis. 2016. PMID: 27293824 Free PMC article.
-
Management of acute postoperative pain with continuous intercostal nerve block after single port video-assisted thoracoscopic anatomic resection.J Thorac Dis. 2016 Dec;8(12):3563-3571. doi: 10.21037/jtd.2016.12.30. J Thorac Dis. 2016. PMID: 28149550 Free PMC article.
-
[Application of thoracoscopy-guided thoracic paravertebral block for analgesia after single-port video-assisted pulmonary lobectomy].Zhonghua Yi Xue Za Zhi. 2020 Sep 8;100(33):2596-2600. doi: 10.3760/cma.j.cn112137-20200525-01647. Zhonghua Yi Xue Za Zhi. 2020. PMID: 32892605 Chinese.
-
Assessment of Intercostal Nerve Block Analgesia for Thoracic Surgery: A Systematic Review and Meta-analysis.JAMA Netw Open. 2021 Nov 1;4(11):e2133394. doi: 10.1001/jamanetworkopen.2021.33394. JAMA Netw Open. 2021. PMID: 34779845 Free PMC article.
-
Paravertebral anaesthesia with or without sedation versus general anaesthesia for women undergoing breast cancer surgery.Cochrane Database Syst Rev. 2021 Feb 25;2(2):CD012968. doi: 10.1002/14651858.CD012968.pub2. Cochrane Database Syst Rev. 2021. PMID: 33629404 Free PMC article.
Cited by
-
Thoracic Paravertebral Block Combined with General Anaesthesia or General Anaesthesia Alone for Thoracoscopic Lung Adenocarcinoma Surgery: A Retrospective Study.Cancer Manag Res. 2022 Mar 3;14:953-965. doi: 10.2147/CMAR.S346285. eCollection 2022. Cancer Manag Res. 2022. PMID: 35264885 Free PMC article.
-
A comparison of the analgesic efficacy of serratus anterior plane block vs. paravertebral nerve block for video-assisted thoracic surgery: a randomized controlled trial.Wideochir Inne Tech Maloinwazyjne. 2022 Mar;17(1):134-142. doi: 10.5114/wiitm.2021.105725. Epub 2021 Apr 30. Wideochir Inne Tech Maloinwazyjne. 2022. PMID: 35251398 Free PMC article.
-
Minimally invasive surgery, precise anesthesia and effective analgesia are crucial for walking within 1 hour after lung surgery.J Thorac Dis. 2024 Sep 30;16(9):5792-5801. doi: 10.21037/jtd-24-685. Epub 2024 Sep 26. J Thorac Dis. 2024. PMID: 39444863 Free PMC article.
-
Pain Management in Minimally Invasive Cardiac Surgery: A Review of Current Clinical Evidence.Pain Ther. 2025 Jun;14(3):913-930. doi: 10.1007/s40122-025-00739-1. Epub 2025 Apr 24. Pain Ther. 2025. PMID: 40272720 Free PMC article. Review.
-
Local anesthetic dosing and toxicity of adult truncal catheters: a narrative review of published practice.Reg Anesth Pain Med. 2024 Mar 4;49(3):209-222. doi: 10.1136/rapm-2023-104667. Reg Anesth Pain Med. 2024. PMID: 37451826 Free PMC article. Review.
References
-
- Lovich-Sapola J, Smith CE, Brandt CP. Postoperative pain control. Surg Clin North Am. 2015;95:301–18. - PubMed
-
- Fiorelli A, Izoo AC, Frongillo EM, et al. Efficacy of wound analgesia for controlling post-thoracotomy pain: a randomized double-blind study. Eur J Cardiothorac Surg. 2016;49:339–47. - PubMed
-
- Kuritzky AM, Aswad BI, Jones RN, et al. Lobectomy by video-assisted thoracic surgery vs muscle-sparing thoracotomy for stage i lung cancer: a critical evaluation of short- and long-term outcomes. J Am Coll Surg. 2015;220:1044–53. - PubMed
-
- Pu Q, Ma L, Mei J, et al. Video-assisted thoracoscopic surgery versus posterolateral thoracotomy lobectomy: a more patient-friendly approach on postoperative pain, pulmonary function andshoulder function. Thoracic Cancer. 2013;4:84–9. - PubMed
-
- American Society of Anesthesiologists Task Force on Acute Pain Management Practice Guidelines for Acute Pain Management in the Perioperative Setting: An Updated Report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology. 2012;116:248–73. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources