

Diagnostic and prognostic capabilities of a biomarker and EMR-based machine learning algorithm for sepsis
- PMID: 33786999
- PMCID: PMC8301583
- DOI: 10.1111/cts.13030
Diagnostic and prognostic capabilities of a biomarker and EMR-based machine learning algorithm for sepsis
Abstract
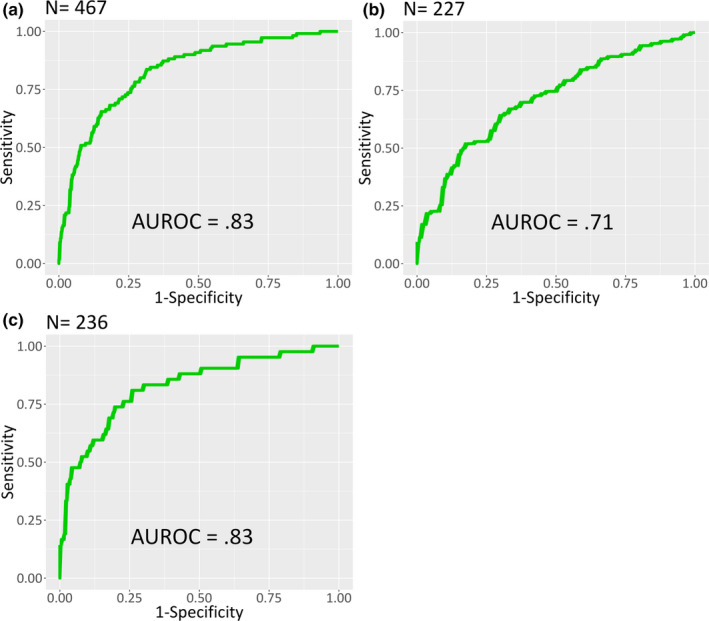
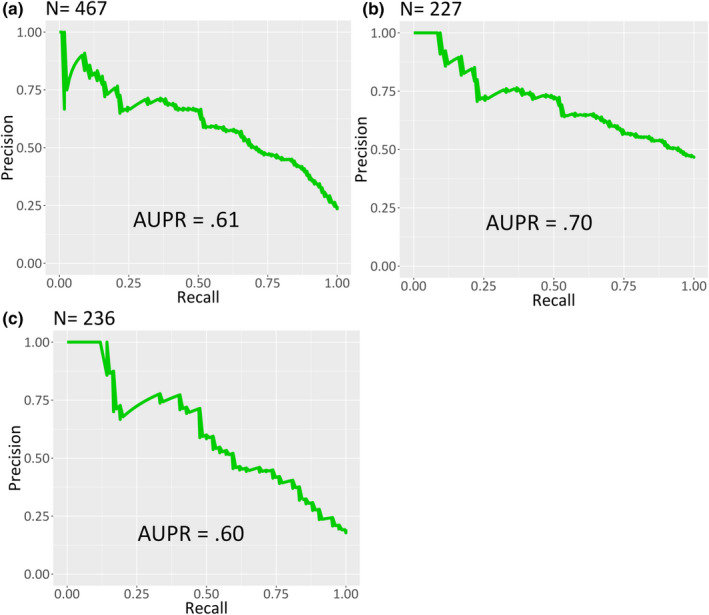
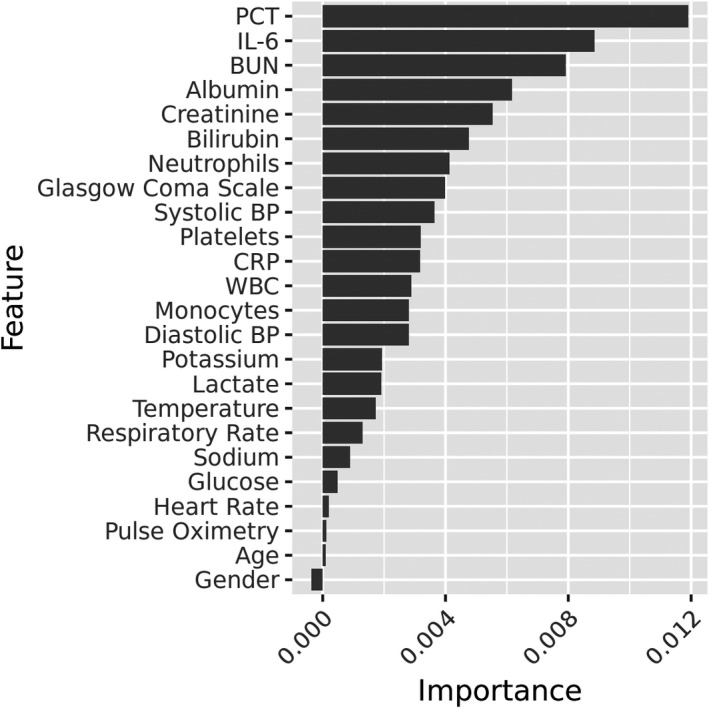
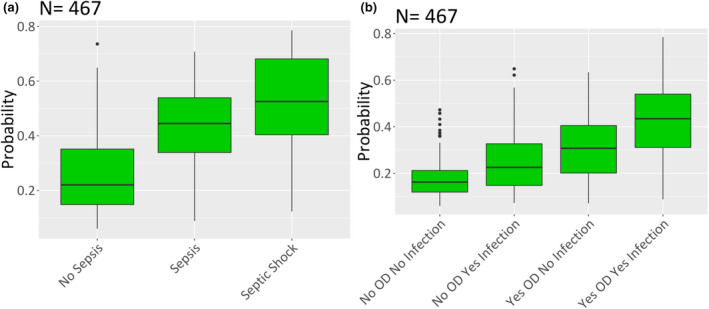
Sepsis is a major cause of mortality among hospitalized patients worldwide. Shorter time to administration of broad-spectrum antibiotics is associated with improved outcomes, but early recognition of sepsis remains a major challenge. In a two-center cohort study with prospective sample collection from 1400 adult patients in emergency departments suspected of sepsis, we sought to determine the diagnostic and prognostic capabilities of a machine-learning algorithm based on clinical data and a set of uncommonly measured biomarkers. Specifically, we demonstrate that a machine-learning model developed using this dataset outputs a score with not only diagnostic capability but also prognostic power with respect to hospital length of stay (LOS), 30-day mortality, and 3-day inpatient re-admission both in our entire testing cohort and various subpopulations. The area under the receiver operating curve (AUROC) for diagnosis of sepsis was 0.83. Predicted risk scores for patients with septic shock were higher compared with patients with sepsis but without shock (p < 0.0001). Scores for patients with infection and organ dysfunction were higher compared with those without either condition (p < 0.0001). Stratification based on predicted scores of the patients into low, medium, and high-risk groups showed significant differences in LOS (p < 0.0001), 30-day mortality (p < 0.0001), and 30-day inpatient readmission (p < 0.0001). In conclusion, a machine-learning algorithm based on electronic medical record (EMR) data and three nonroutinely measured biomarkers demonstrated good diagnostic and prognostic capability at the time of initial blood culture.
© 2021 The Authors. Clinical and Translational Science published by Wiley Periodicals LLC on behalf of the American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
I.T., G.L.D., C.L.E., S.K., L.S., S.S.T., L.Q., S.M., B.R.J., and R.B. have financial interests in Prenosis Inc. All other authors declared no competing interests for this work.
Figures

References
-
- Ferrer R, Martin‐Loeches I, Phillips G, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour. Crit Care Med. 2014;42:1749‐1755. - PubMed
-
- Gaieski DF, Mikkelsen ME, Band RA, et al. Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal‐directed therapy was initiated in the emergency department. Crit Care Med. 2010;38:1045‐1053. - PubMed
-
- Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34:1589‐1596. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
