

The New Bern Chondrolabral Classification Is Reliable and Reproducible
- PMID: 33787519
- PMCID: PMC8083824
- DOI: 10.1097/CORR.0000000000001706
The New Bern Chondrolabral Classification Is Reliable and Reproducible
Abstract
Background: Several classification systems have been used to describe early lesions of hip cartilage and the acetabular labrum in young adults with hip pain. Some of them were introduced before the concept of femoroacetabular impingement was proposed. Others were developed for other joints (such as the patellofemoral joint). However, these often demonstrate inadequate reliability, and they do not characterize all possible lesions. Therefore, we developed a novel classification system.
Question/purpose: We asked: What is the (1) intraobserver reliability, (2) interobserver reproducibility, and (3) percentage of nonclassifiable lesions of the new classification system for damage to the hip cartilage and labrum compared with six established classification systems for chondral lesions (Beck et al. [4], Konan et al. [10], Outerbridge et al. [14]) and labral lesions (Beck et al. [3], Lage et al. [12], Peters and Erickson [15])?
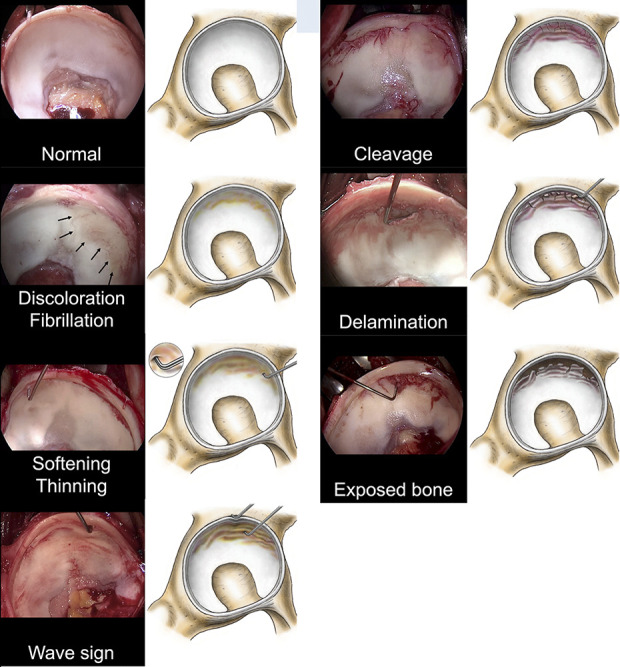
Methods: We performed a validation study of a new classification system of early chondrolabral degeneration lesions based on intraoperative video documentation taken during surgical hip dislocations for joint-preserving surgery in 57 hips (56 patients) performed by one surgeon with standard video documentation of intraarticular lesions. The exclusion criteria were low-quality videos, inadequate exposure angles, traumatic lesions, and incomplete radiographic documentation. This left 42 hips (41 patients) for the blinded and randomized analysis of six raters, including those with cam-pincer-type femoroacetabular impingement (FAI) (19 hips in 18 patients), isolated cam-type FAI (10 hips), extraarticular FAI due to femoral anteversion (seven hips), isolated pincer-type FAI (two hips), focal avascular necrosis (two hips), localized pigmented villonodular synovitis (one hip), and acetabular dysplasia as a sequelae of Perthes disease (one hip). The raters had various degrees of experience in hip surgery: Three were board-certified orthopaedic fellows and three were orthopaedic residents, in whom we chose to prove the general usability of the classification systems in less experienced readers. Every rater was given the original publication of all existing classification systems and a visual guide of the new Bern classification system. Every rater classified the lesions according the existing classifications (cartilage: Beck et al. [4], Konan et al. [10], and Outerbridge et al. [14]; labrum: Beck et al. [3], Peters and Erickson [15], and Lage et al. [12]) and our new Bern chondrolabral classification system. The intraclass correlation coefficient with 95% confidence interval was used to assess the intraobserver reliability and interobserver reproducibility. The percentage of nonclassifiable lesions was calculated as an absolute number and percentage.
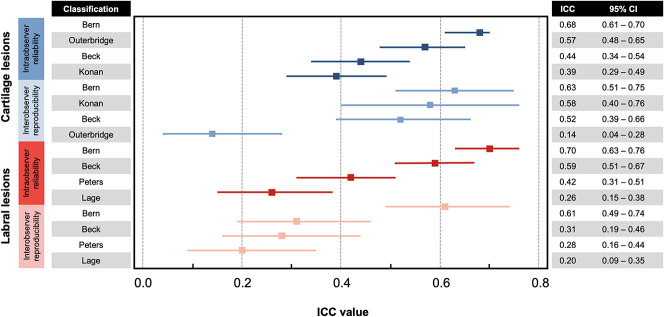
Results: The intraobserver intercorrelation coefficients (ICCs) for cartilage lesions were as follows: the Bern classification system (0.68 [95% CI 0.61 to 0.70]), Beck (0.44 [95% CI 0.34 to 0.54]), Konan (0.39 [95% CI 0.29 to 0.49]), and the Outerbridge classification (0.57 [95% CI 0.48 to 0.65]). For labral lesions, the ICCs were as follows: the Bern classification (0.70 [95% CI 0.63 to 0.76]), Peters (0.42 [95% CI 0.31 to 0.51]), Lage (0.26 [95% CI 0.15 to 0.38]), and Beck (0.59 [95% CI 0.51 to 0.67]). The interobserver ICCs for cartilage were as follows: the Bern classification system (0.63 [95% CI 0.51 to 0.75), the Outerbridge (0.14 [95% CI 0.04 to 0.28]), Konan (0.58 [95% CI 0.40 to 0.76]), and Beck (0.52 [95% CI 0.39 to 0.66]). For labral lesions, the ICCs were as follows: the Bern classification (0.61 [95% CI 0.49 to 0.74]), Beck (0.31 [95% CI 0.19 to 0.46]), Peters (0.28 [95% CI 0.16 to 0.44]), and Lage (0.20 [95% CI 0.09 to 0.35]). The percentage of nonclassifiable cartilage lesions was 0% for the Bern, 0.04% for Beck, 17% for Konan, and 25% for the Outerbridge classification. The percentage of nonclassifiable labral lesions was 0% for Bern and Beck, 4% for Peters, and 25% for Lage.
Conclusion: We have observed some shortcomings with currently used classification systems for hip pathology, and the new classification system we developed seems to have improved the intraobserver reliability compared with the Beck and Konan classifications in cartilage lesions and with the Peters and Lage classifications in labral lesions. The interrater reproducibility of the Bern classification seems to have improved in cartilage lesions compared with the Outerbridge classification and in labral lesions compared with the Beck, Peters, and Lage classifications. The Bern classification identified all present cartilage and labral lesions. It provides a solid clinical basis for accurate descriptions of early degenerative hip lesions independent of etiology, and it is reproducible enough to use in the reporting of clinical research. Further studies need to replicate our findings in the hands of nondevelopers and should focus on the prognostic value of this classification and its utility in guiding surgical indications.
Level of evidence: Level II, diagnostic study.
Copyright © 2021 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that neither he nor she, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures

Comment in
-
CORR Insights®: The New Bern Chondrolabral Classification is Reliable and Reproducible.Clin Orthop Relat Res. 2021 May 1;479(5):1014-1015. doi: 10.1097/CORR.0000000000001770. Clin Orthop Relat Res. 2021. PMID: 33835098 Free PMC article. No abstract available.
References
-
- Amenabar T, Piriz J, Mella C, Hetaimish B, O’Donnell J. Reliability of 3 different arthroscopic classifications for chondral damage of the acetabulum. Arthroscopy. 2015;31:1492-1496. - PubMed
-
- Beck Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005;87:1012-1018. - PubMed
-
- Beck M, Leunig M, Parvizi J, Boutier V, Wyss D, Ganz R. Anterior femoroacetabular impingement: part II. Midterm results of surgical treatment. Clin Orthop Relat Res . 2004;418:67-73. - PubMed
-
- Bonett DG. Sample size requirements for testing and estimating coefficient alpha. J Educ Behav Stat. 2002;27:335-340.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
