

Microablative fractional radiofrequency as a therapeutic option for vulvar lichen sclerosus: a pilot study
- PMID: 33787656
- PMCID: PMC7978666
- DOI: 10.6061/clinics/2021/e2567
Microablative fractional radiofrequency as a therapeutic option for vulvar lichen sclerosus: a pilot study
Abstract
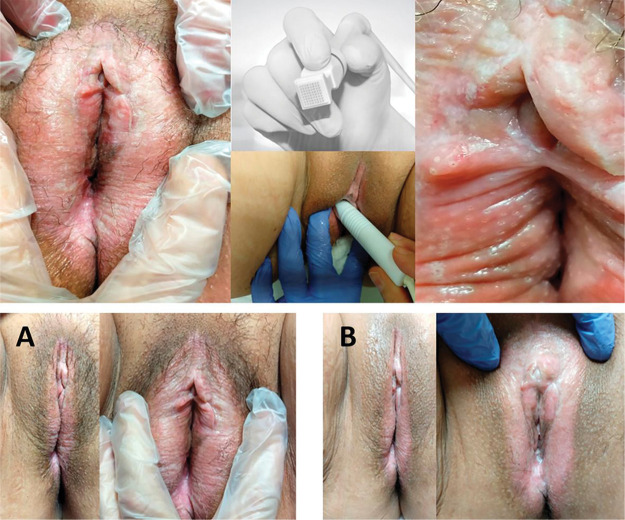
Objectives: To assess the clinical response to and the histomorphometric effects of microablative fractional radiofrequency (MFR) in women with symptomatic vulvar lichen sclerosus (VLS).
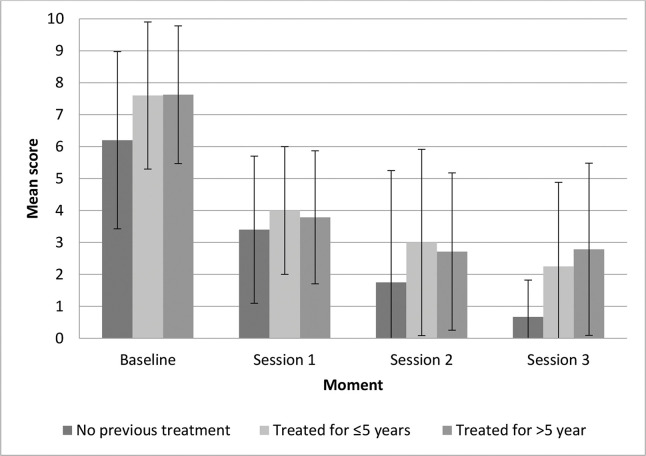
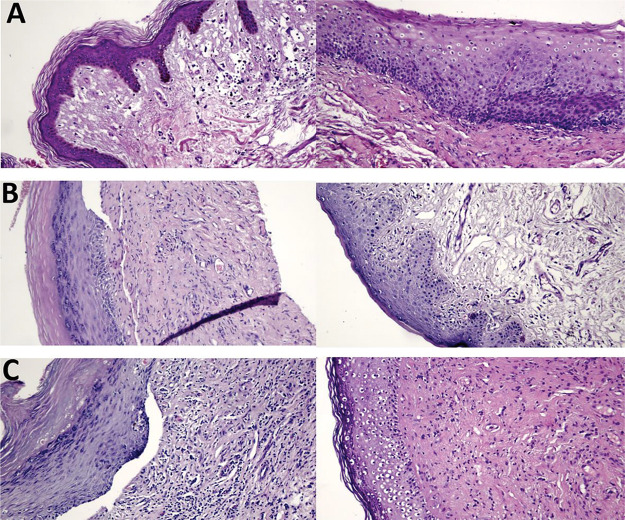
Methods: This was a pilot study on the use of MFR for the treatment of VLS. Upon recruitment and at each treatment session, all participants were examined and each of their symptoms were rated on a visual analog scale. After the procedure, the participants completed a satisfaction questionnaire. We compared the morphometric findings of vulvar biopsies performed at enrollment and after the last treatment session. The participants were divided into three groups according to previous treatment with corticosteroids: G1, no previous treatment; G2, treated for up to 5 years; and G3, treated for >5 years.
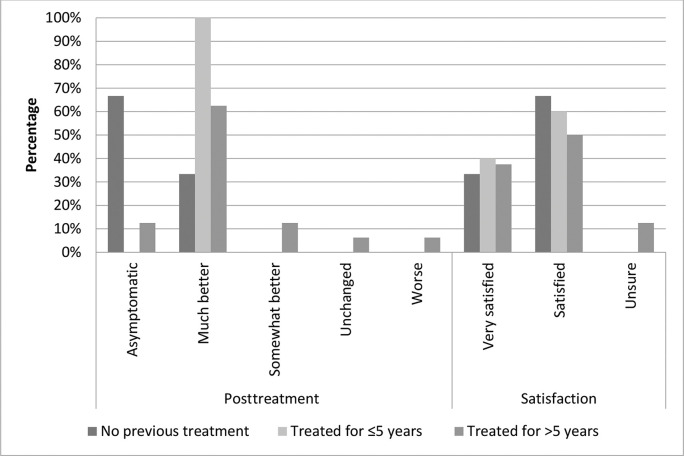
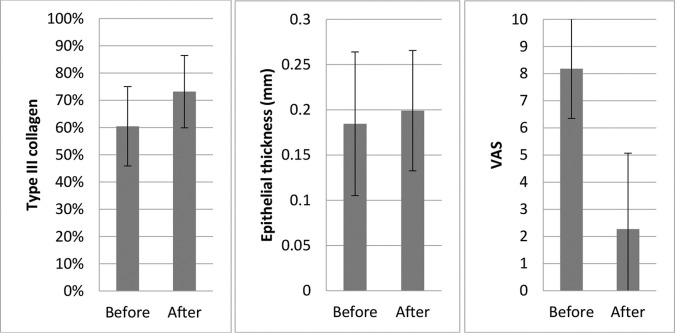
Results: This study included 26 women. After two to three sessions, most participants in all groups became either "asymptomatic" or "much better" than before treatment and were "very satisfied" or "satisfied" with the intervention. Pruritus and burning sensation were the most frequently reported symptoms. Nearly 40% of the participants in all groups reported complete remission of symptoms. The improvement was rated as moderate or higher by 80%, 76%, and 66% of the women in groups 1, 2, and 3, respectively. The improvement of symptoms persisted for 11 months (range, 7-16 months), on average, after the treatment. Type III collagen concentration significantly increased and was associated with important symptom improvement. Tissue trophism and vascularization also increased but did not reach statistical significance, probably because of the small number of cases.
Conclusions: MFR may be an effective and safe treatment for symptomatic VLS.
Conflict of interest statement
No potential conflict of interest was reported.
Figures
References
-
- Caussade A. Liquen escleroso: actualización. Arch Ginecol Obstet. 2019;57(1):31.
-
- Goldstein AT, Marinoff SC, Christopher K, Srodon M. Prevalence of vulvar lichen sclerosus in a general gynecology practice. J Reprod Med. 2005;50(7):477–80. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
