

Comparative Efficacy and Relative Ranking of Biologics and Oral Therapies for Moderate-to-Severe Plaque Psoriasis: A Network Meta-analysis
- PMID: 33788177
- PMCID: PMC8163943
- DOI: 10.1007/s13555-021-00511-1
Comparative Efficacy and Relative Ranking of Biologics and Oral Therapies for Moderate-to-Severe Plaque Psoriasis: A Network Meta-analysis
Abstract
Introduction: The clinical benefits of biologic and oral treatments for moderate-to-severe plaque psoriasis are well-established, but efficacy outcomes can vary across therapies. Comparative efficacy analysis can be highly informative in clinical settings with multiple therapeutic options. This study assessed the short-term and long-term comparative efficacy of biologic and oral treatments for moderate-to-severe psoriasis.
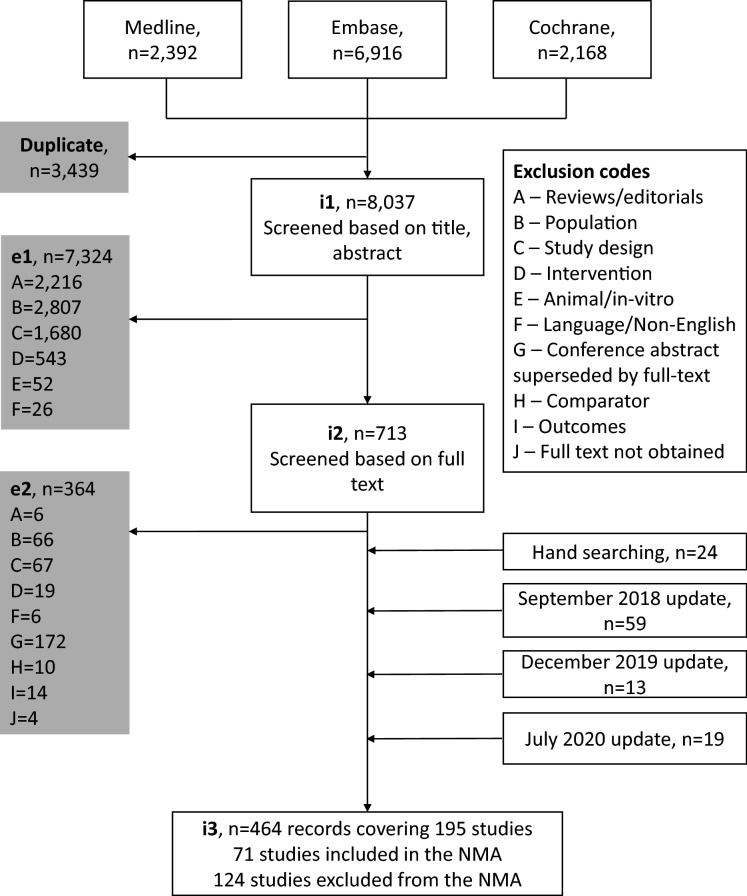
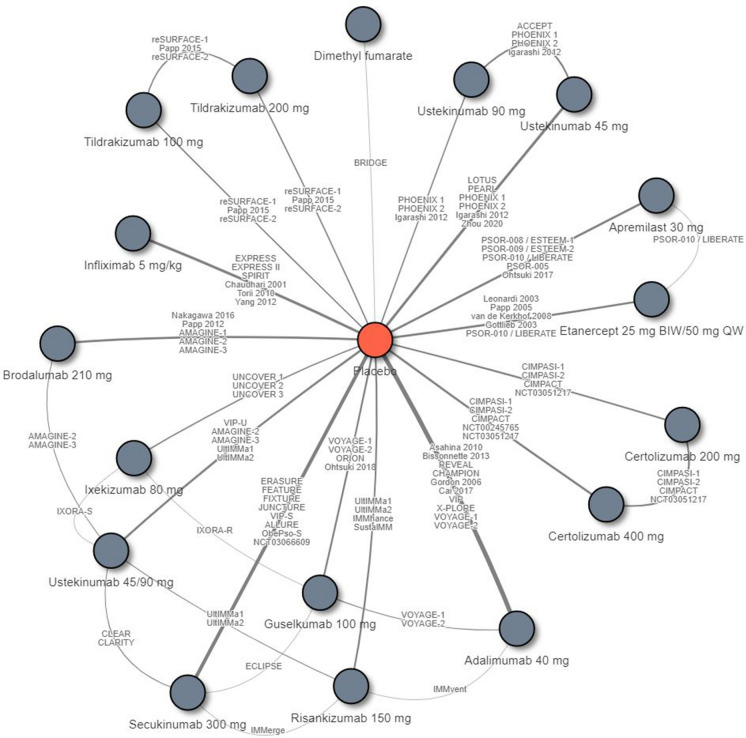
Methods: A systematic literature review identified phase 2/3/4 randomized controlled trials (RCTs) through to 1 July 2020 for Food and Drug Administration- or European Medicines Agency-licensed treatments for moderate-to-severe psoriasis. Psoriasis Area and Severity Index (PASI) 75/90/100 response rates at the end of the primary response (short-term: 10-16 weeks from baseline) and maintenance periods (long-term: 48-52 weeks from baseline) were estimated using Bayesian network meta-analysis. Surfaces under the cumulative ranking curves (SUCRA) were estimated to present the relative ranking of treatments.
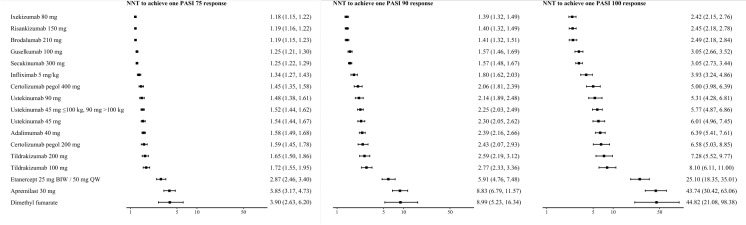
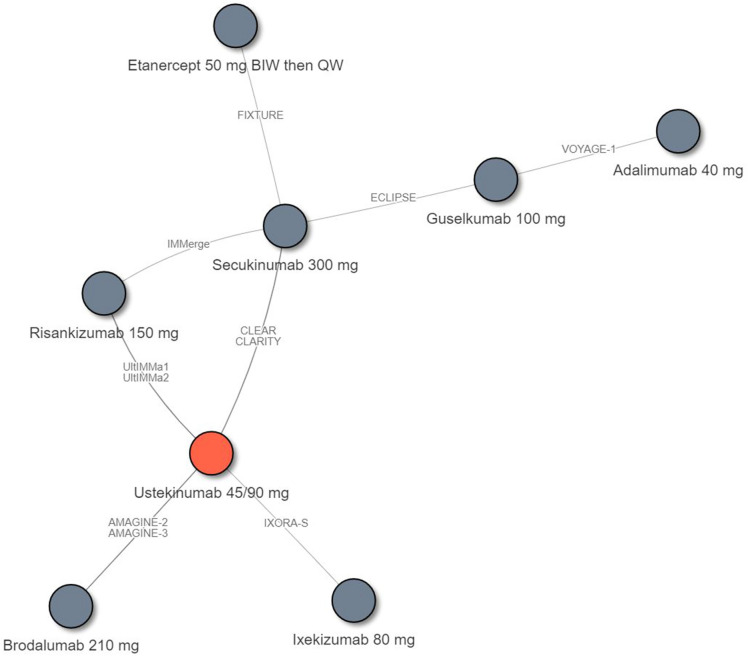
Results: In the short term (N = 71 RCTs), the PASI 90 response rates were highest for ixekizumab (72.9%, SUCRA 0.951), risankizumab (72.5%, 0.940), and brodalumab (72.0%, 0.930), which were significantly higher than those for guselkumab (65.0%, 0.795), secukinumab (65.0%, 0.794), infliximab (56.8%, 0.702), certolizumab (400 mg: 49.6%, 0.607; 200 mg: 42.2%, 0.389), ustekinumab (90 mg: 47.9%, 0.568; weight-based: 45.7%, 0.505; 45 mg: 44.6%, 0.460), adalimumab (43.0%, 0.410), tildrakizumab (200 mg: 39.7%, 0.327; 100 mg: 37.2%, 0.268), etanercept (18.0%, 0.171), apremilast (12.4%, 0.090), and dimethyl fumarate (12.2%, 0.092). The PASI 100 response rates were highest for ixekizumab (41.4%), risankizumab (40.8%), and brodalumab (40.3%). In the long term (N = 11 RCTs), the PASI 90 rate was highest for risankizumab (85.3%, SUCRA: 0.998), which were significantly higher than those for brodalumab (78.8%, 0.786), guselkumab (78.1%, 0.760), ixekizumab (72.1%, 0.577), secukinumab (67.0%, 0.450), ustekinumab (weight-based: 55.0%, 0.252), adalimumab (51.6%, 0.176), and etanercept (37.9%, 0.001). Risankizumab had the highest PASI 100 response rate (65.4%), followed by brodalumab (55.7%) and guselkumab (54.8%).
Conclusions: Ixekizumab, risankizumab, and brodalumab had the highest short-term efficacy, and risankizumab had the highest long-term efficacy.
Keywords: Biologic therapies; Network meta-analysis; Plaque psoriasis.
Figures
References
-
- Ighani A, Partridge ACR, Shear NH, Lynde C, Gulliver WP, Sibbald C, et al. Comparison of management guidelines for moderate-to-severe plaque psoriasis: a review of phototherapy, systemic therapies, and biologic agents. J Cutan Med Surg. 2019;23(2):204–221. - PubMed
-
- Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis: a review. JAMA. 2020;323(19):1945–1960. - PubMed
-
- Elewski BE, Puig L, Mordin M, Gilloteau I, Sherif B, Fox T, et al. Psoriasis patients with psoriasis Area and Severity Index (PASI) 90 response achieve greater health-related quality-of-life improvements than those with PASI 75-89 response: results from two phase 3 studies of secukinumab. J Dermatol Treat. 2017;28(6):492–499. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
