

Clinical characteristics and outcomes for 7,995 patients with SARS-CoV-2 infection
- PMID: 33788846
- PMCID: PMC8011821
- DOI: 10.1371/journal.pone.0243291
Clinical characteristics and outcomes for 7,995 patients with SARS-CoV-2 infection
Abstract
Objective: Severe acute respiratory syndrome virus (SARS-CoV-2) has infected millions of people worldwide. Our goal was to identify risk factors associated with admission and disease severity in patients with SARS-CoV-2.
Design: This was an observational, retrospective study based on real-world data for 7,995 patients with SARS-CoV-2 from a clinical data repository.
Setting: Yale New Haven Health (YNHH) is a five-hospital academic health system serving a diverse patient population with community and teaching facilities in both urban and suburban areas.
Populations: The study included adult patients who had SARS-CoV-2 testing at YNHH between March 1 and April 30, 2020.
Main outcome and performance measures: Primary outcomes were admission and in-hospital mortality for patients with SARS-CoV-2 infection as determined by RT-PCR testing. We also assessed features associated with the need for respiratory support.
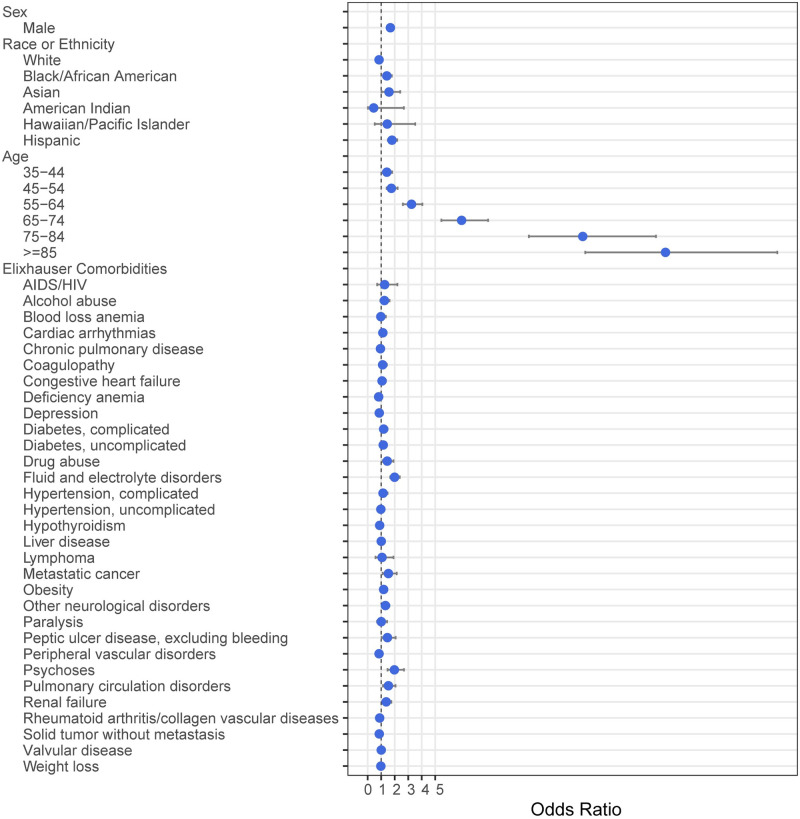
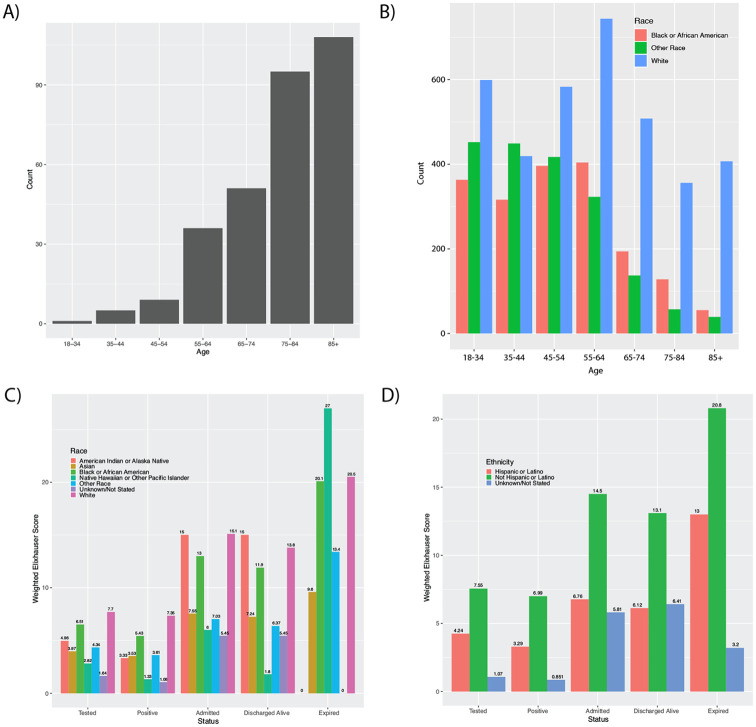
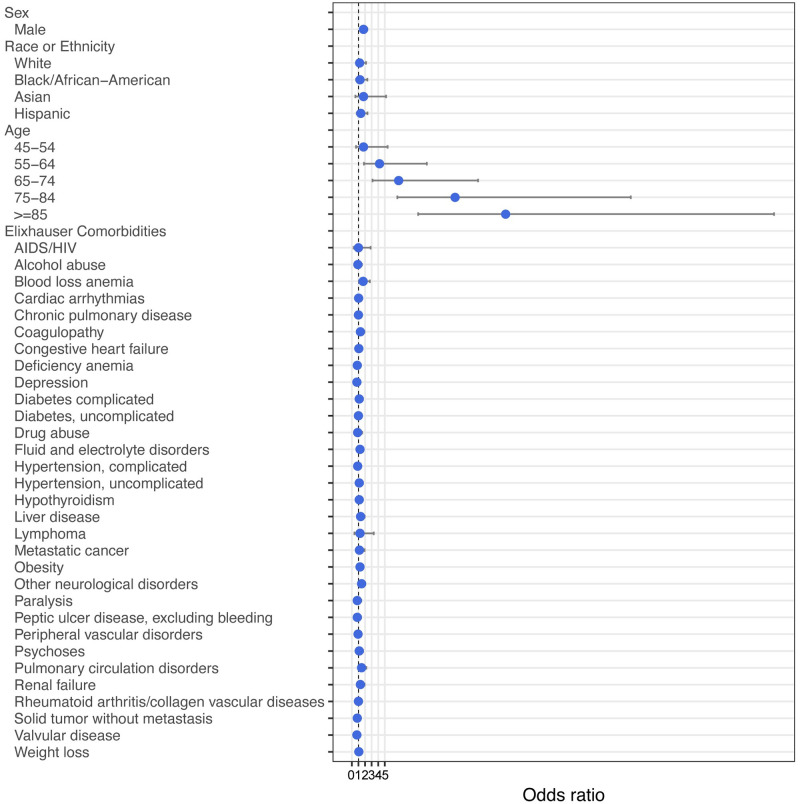
Results: Of the 28605 patients tested for SARS-CoV-2, 7995 patients (27.9%) had an infection (median age 52.3 years) and 2154 (26.9%) of these had an associated admission (median age 66.2 years). Of admitted patients, 2152 (99.9%) had a discharge disposition at the end of the study period. Of these, 329 (15.3%) required invasive mechanical ventilation and 305 (14.2%) expired. Increased age and male sex were positively associated with admission and in-hospital mortality (median age 80.7 years), while comorbidities had a much weaker association with the risk of admission or mortality. Black race (OR 1.43, 95%CI 1.14-1.78) and Hispanic ethnicity (OR 1.81, 95%CI 1.50-2.18) were identified as risk factors for admission, but, among discharged patients, age-adjusted in-hospital mortality was not significantly different among racial and ethnic groups.
Conclusions: This observational study identified, among people testing positive for SARS-CoV-2 infection, older age and male sex as the most strongly associated risks for admission and in-hospital mortality in patients with SARS-CoV-2 infection. While minority racial and ethnic groups had increased burden of disease and risk of admission, age-adjusted in-hospital mortality for discharged patients was not significantly different among racial and ethnic groups. Ongoing studies will be needed to continue to evaluate these risks, particularly in the setting of evolving treatment guidelines.
Conflict of interest statement
H.M.K. works under contract with the Centers for Medicare & Medicaid Services to support quality measurement programs; was a recipient of a research grant, through Yale, from Medtronic and the U.S. Food and Drug Administration to develop methods for post-market surveillance of medical devices; was a recipient of a research grant from Johnson & Johnson, through Yale University, to support clinical trial data sharing; was a recipient of a research agreement, through Yale University, from the Shenzhen Center for Health Information for work to advance intelligent disease prevention and health promotion; collaborates with the National Center for Cardiovascular Diseases in Beijing; receives payment from the Arnold & Porter Law Firm for work related to the Sanofi clopidogrel litigation, from the Martin Baughman Law Firm for work related to the Cook Celect IVC filter litigation, and from the Siegfried and Jensen Law Firm for work related to Vioxx litigation; chairs a Cardiac Scientific Advisory Board for UnitedHealth; was a member of the IBM Watson Health Life Sciences Board; is a member of the Advisory Board for Element Science, the Advisory Board for Facebook, and the Physician Advisory Board for Aetna; and is the co-founder of HugoHealth, a personal health information platform, and cofounder of Refactor Health, a healthcare AI-augmented data management company. W.L.S. was an investigator for a research agreement, through Yale University, from the Shenzhen Center for Health Information for work to advance intelligent disease prevention and health promotion; collaborates with the National Center for Cardiovascular Diseases in Beijing; is a technical consultant to HugoHealth, a personal health information platform, and cofounder of Refactor Health, an AI-augmented data management platform for healthcare; is a consultant for Interpace Diagnostics Group, a molecular diagnostics company. This does not alter our adherence to PLOS ONE policies on sharing data and materials. There are no patents, products in development or marketed products associated with this research to declare.
Figures
Update of
-
Clinical Characteristics and Outcomes for 7,995 Patients with SARS-CoV-2 Infection.medRxiv [Preprint]. 2020 Nov 8:2020.07.19.20157305. doi: 10.1101/2020.07.19.20157305. medRxiv. 2020. Update in: PLoS One. 2021 Mar 31;16(3):e0243291. doi: 10.1371/journal.pone.0243291. PMID: 32743602 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
