

The long-term impact of the Leprosy Post-Exposure Prophylaxis (LPEP) program on leprosy incidence: A modelling study
- PMID: 33788863
- PMCID: PMC8011751
- DOI: 10.1371/journal.pntd.0009279
The long-term impact of the Leprosy Post-Exposure Prophylaxis (LPEP) program on leprosy incidence: A modelling study
Abstract
Background: The Leprosy Post-Exposure Prophylaxis (LPEP) program explored the feasibility and impact of contact tracing and the provision of single dose rifampicin (SDR) to eligible contacts of newly diagnosed leprosy patients in Brazil, India, Indonesia, Myanmar, Nepal, Sri Lanka and Tanzania. As the impact of the programme is difficult to establish in the short term, we apply mathematical modelling to predict its long-term impact on the leprosy incidence.
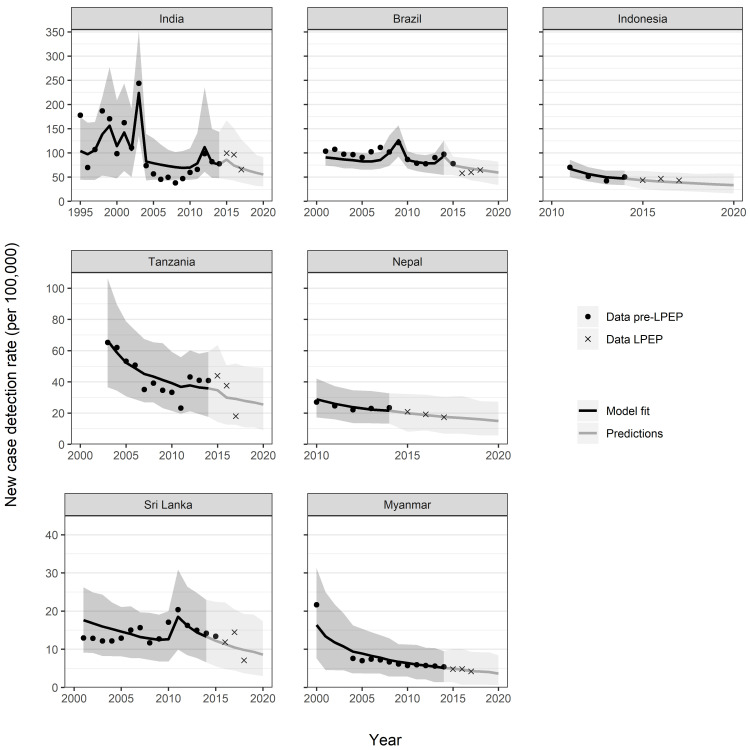
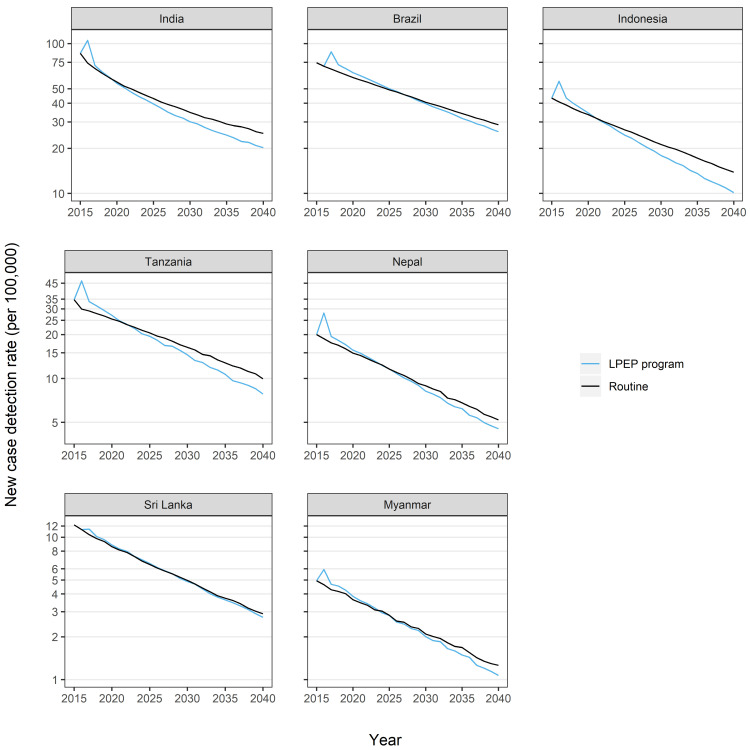
Methodology: The individual-based model SIMCOLEP was calibrated and validated to the historic leprosy incidence data in the study areas. For each area, we assessed two scenarios: 1) continuation of existing routine activities as in 2014; and 2) routine activities combined with LPEP starting in 2015. The number of contacts per index patient screened varied from 1 to 36 between areas. Projections were made until 2040.
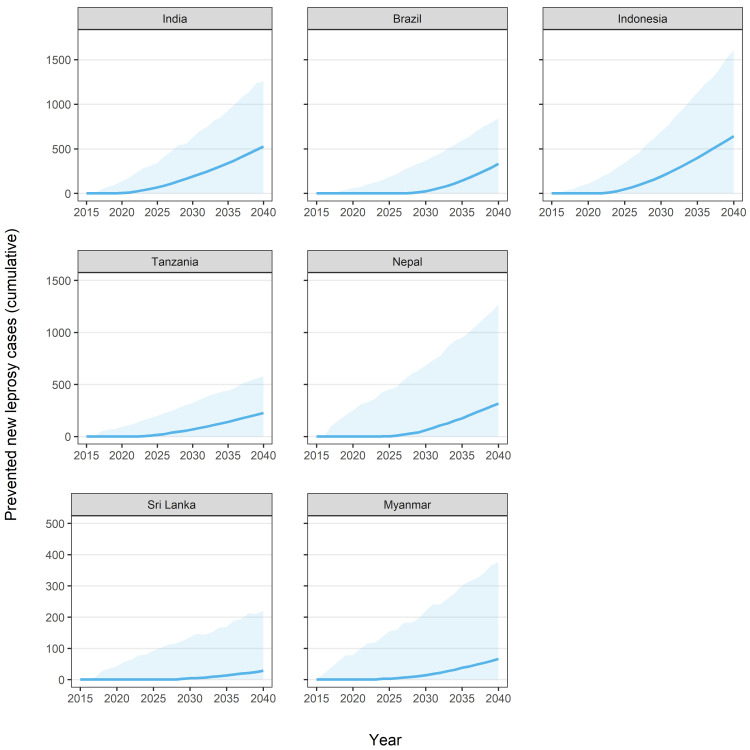
Principal findings: In all areas, the LPEP program increased the number of detected cases in the first year(s) of the programme as compared to the routine programme, followed by a faster reduction afterwards with increasing benefit over time. LPEP could accelerate the reduction of the leprosy incidence by up to six years as compared to the routine programme. The impact of LPEP varied by area due to differences in the number of contacts per index patient included and differences in leprosy epidemiology and routine control programme.
Conclusions: The LPEP program contributes significantly to the reduction of the leprosy incidence and could potentially accelerate the interruption of transmission. It would be advisable to include contact tracing/screening and SDR in routine leprosy programmes.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: Novartis Foundation and International Federation of Anti-Leprosy Association partners provided technical input in the design phase of the LPEP program and ensured overall programme coordination. All authors are either staff of the Novartis Foundation (Arielle Cavaliero, Zaahira Gani, and Ann Aerts), work as paid consultants for the programme described here (David J Blok, Peter Steinmann, Anuj Tiwari, Tanja Barth-Jaeggi, Marc Bonenberger, Helena Grete, Christa Kasang, Liesbeth Mieras, Unnati R Saha, Wim H van Brakel, Bart Vander Plaetse, and Jan Hendrik Richardus), act as national programme coordinators (Mohammad A Arif, Nand Lal Banstola, Rabindra Baskota, Teky Budiawan, Eliane Ignotti, Deusdedit V Kamara, Pratap R Manglani, Blasdus F Njako, Tiara Pakasi, Nayani D Suriyarachchi, Aye Tin Maung, Tin Shwe, and Millawage S D Wijesinghe) or serve on the Steering Committee of the programme (David Blaney, Paul Saunderson, W Cairns S Smith, René Stäheli, Jan van Berkel, Marcos Virmond). The funder had no role in the interpretation of findings or decision to publish this manuscript. Author Aye Tin Maung was unavailable to confirm his authorship contributions. On his behalf, the corresponding author has reported his contributions to the best of his knowledge.
Figures
References
-
- Hatta M, van Beers SM, Madjid B, Djumadi A, de Wit MY, Klatser PR. Distribution and persistence of Mycobacterium leprae nasal carriage among a population in which leprosy is endemic in Indonesia. Trans R Soc Trop Med Hyg. 1995;89(4):381–5. Epub 1995/07/01. 10.1016/0035-9203(95)90018-7 . - DOI - PubMed
-
- Bratschi MW, Steinmann P, Wickenden A, Gillis TP. Current knowledge on Mycobacterium leprae transmission: a systematic literature review. Lepr Rev. 2015;86(2):142–55. Epub 2015/10/28. . - PubMed
-
- Moet FJ, Pahan D, Schuring RP, Oskam L, Richardus JH. Physical distance, genetic relationship, age, and leprosy classification are independent risk factors for leprosy in contacts of patients with leprosy. J Infect Dis. 2006;193(3):346–53. Epub 2006/01/03. JID35096 [pii] 10.1086/499278 . - DOI - PubMed
-
- WHO. Global leprosy update, 2018: moving towards a leprosy-free world. Wkly Epidemiol Rec. 2019;94(35/36):389–412 10.1002/jcp.1040860303 - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
