

24 hour consultant obstetrician presence on the labour ward and intrapartum outcomes in a large unit in England: A time series analysis
- PMID: 33788880
- PMCID: PMC8011758
- DOI: 10.1371/journal.pone.0249233
24 hour consultant obstetrician presence on the labour ward and intrapartum outcomes in a large unit in England: A time series analysis
Abstract
Objectives: To explore the effect of introducing 24/7 resident labour ward consultant presence on neonatal and maternal outcomes in a large obstetric unit in England.
Design: Retrospective time sequence analysis of routinely collected data.
Setting: Obstetric unit of large teaching hospital in England.
Participants: Women and babies delivered between1 July 2011 and 30 June 2017. Births <24 weeks gestation or by planned caesarean section were excluded.
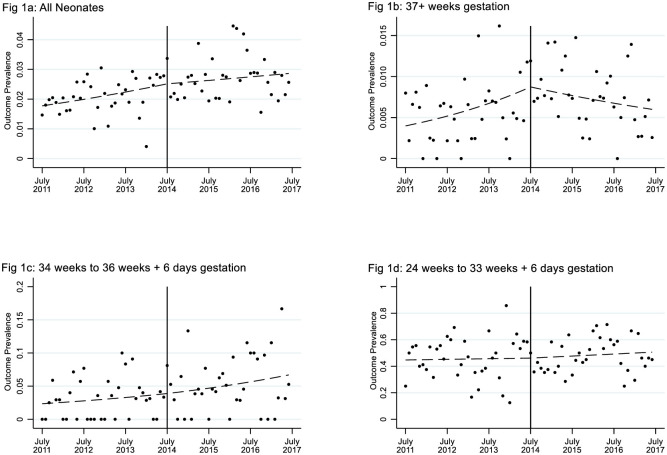
Main outcome measures: The primary composite outcome comprised intrapartum stillbirth, neonatal death, babies requiring therapeutic hypothermia, or admission to neonatal intensive care within three hours of birth. Secondary outcomes included markers of neonatal and maternal morbidity. Planned subgroup analyses investigated gestation (<34 weeks; 34-36 weeks; ≥37 weeks) and time of day.
Results: 17324 babies delivered before and 16110 after 24/7 consultant presence. The prevalence of the primary outcome increased by 0.65%, from 2.07% (359/17324) before 24/7 consultant presence to 2.72% (438/16110, P < 0.001) after 24/7 consultant presence which was consistent with an upward trend over time already well established before 24/7 consultant presence began (OR 1.09 p.a.; CI 1.04 to 1.13). Overall, there was no change in this trend associated with the transition to 24/7. However, in babies born ≥37 weeks gestation, the upward trend was reversed after implementation of 24/7 (OR 0.67 p.a.; CI 0.49 to 0.93; P = 0.017). No substantial differences were shown in other outcomes or subgroups.
Conclusions: Overall, resident consultant obstetrician presence 24/7 on labour ward was not associated with a change in a pre-existing trend of increasing adverse infant outcomes. However, 24/7 presence was associated with a reversal in increasing adverse outcomes for term babies.
Conflict of interest statement
Sharon Morad reports that she is married to one of the co-authors (DP). David Pitches reports that he is married to the corresponding author (SM). Alan Girling has nothing to disclose. Vikki Fradd has nothing to disclose. Beck Taylor reports funding from the NIHR during the study duration. Christine MacArthur reports funding from the NIHR during the study duration. Sara Kenyon reports funding from the NIHR during the study duration. Our competing interests statement does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Birth "Out-of-Hours": An Evaluation of Obstetric Practice and Outcome According to the Presence of Senior Obstetricians on the Labour Ward.PLoS Med. 2016 Apr 19;13(4):e1002000. doi: 10.1371/journal.pmed.1002000. eCollection 2016 Apr. PLoS Med. 2016. PMID: 27093698 Free PMC article.
-
Maternal and newborn outcomes with elective induction of labor at term.Am J Obstet Gynecol. 2019 Mar;220(3):273.e1-273.e11. doi: 10.1016/j.ajog.2019.01.223. Epub 2019 Feb 17. Am J Obstet Gynecol. 2019. PMID: 30716284
-
The risk of intrapartum/neonatal mortality and morbidity following birth at 37 weeks of gestation: a nationwide cohort study.BJOG. 2019 Sep;126(10):1252-1257. doi: 10.1111/1471-0528.15748. Epub 2019 Apr 24. BJOG. 2019. PMID: 30946519 Free PMC article.
-
Maternal and neonatal outcomes after implementation of a hospital policy to limit low-risk planned caesarean deliveries before 39 weeks of gestation: an interrupted time-series analysis.BJOG. 2015 Aug;122(9):1200-6. doi: 10.1111/1471-0528.13396. Epub 2015 Apr 8. BJOG. 2015. PMID: 25851865
-
Hiding in plain sight: Inconvenient facts for patient safety in non-24/7 theatre on-site staffed obstetric units.Aust N Z J Obstet Gynaecol. 2023 Aug;63(4):606-611. doi: 10.1111/ajo.13701. Aust N Z J Obstet Gynaecol. 2023. PMID: 37555707 Review.
Cited by
-
Schizoaffective Disorder and Concurrent Rhabdomyolysis.Cureus. 2021 Nov 25;13(11):e19896. doi: 10.7759/cureus.19896. eCollection 2021 Nov. Cureus. 2021. PMID: 34976507 Free PMC article.
References
-
- NPEU. MBRRACE-UK: Mothers and Babies: Reducing Risk through Audits and Confidential Enquiries across the UK. [Internet]. Oxford: NPEU; [updated 2021 Jan 14; cited 2021 Feb 01]. https://www.npeu.ox.ac.uk/mbrrace-uk/reports.
-
- National Patient Safety Association, 2006 quoted in RCOG, Safer Childbirth: Minimum standards for the organisation and delivery of care in labour. 2007, London: RCOG Press
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
