

Characterizing COVID-19 clinical phenotypes and associated comorbidities and complication profiles
- PMID: 33788884
- PMCID: PMC8011766
- DOI: 10.1371/journal.pone.0248956
Characterizing COVID-19 clinical phenotypes and associated comorbidities and complication profiles
Abstract
Purpose: Heterogeneity has been observed in outcomes of hospitalized patients with coronavirus disease 2019 (COVID-19). Identification of clinical phenotypes may facilitate tailored therapy and improve outcomes. The purpose of this study is to identify specific clinical phenotypes across COVID-19 patients and compare admission characteristics and outcomes.
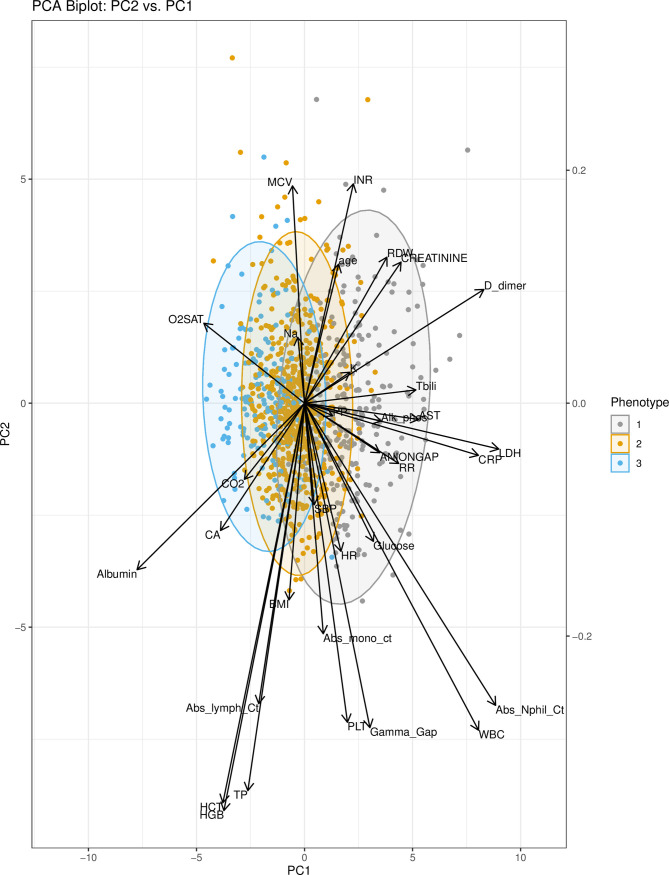
Methods: This is a retrospective analysis of COVID-19 patients from March 7, 2020 to August 25, 2020 at 14 U.S. hospitals. Ensemble clustering was performed on 33 variables collected within 72 hours of admission. Principal component analysis was performed to visualize variable contributions to clustering. Multinomial regression models were fit to compare patient comorbidities across phenotypes. Multivariable models were fit to estimate associations between phenotype and in-hospital complications and clinical outcomes.
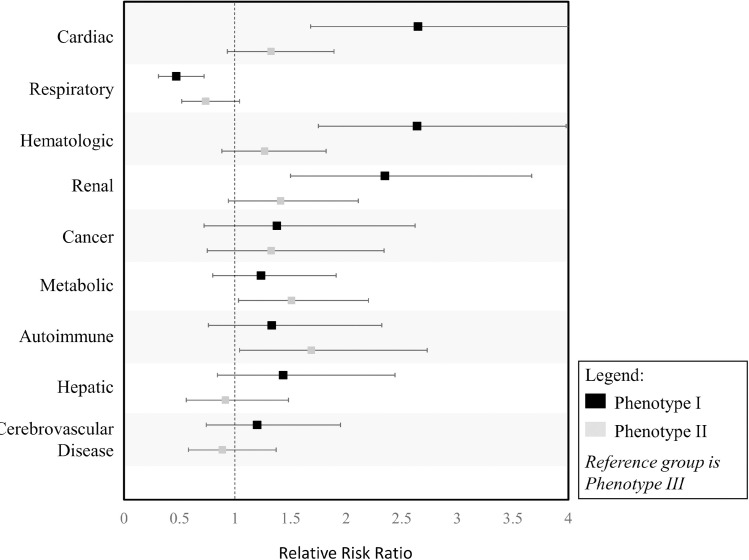
Results: The database included 1,022 hospitalized patients with COVID-19. Three clinical phenotypes were identified (I, II, III), with 236 [23.1%] patients in phenotype I, 613 [60%] patients in phenotype II, and 173 [16.9%] patients in phenotype III. Patients with respiratory comorbidities were most commonly phenotype III (p = 0.002), while patients with hematologic, renal, and cardiac (all p<0.001) comorbidities were most commonly phenotype I. Adjusted odds of respiratory, renal, hepatic, metabolic (all p<0.001), and hematological (p = 0.02) complications were highest for phenotype I. Phenotypes I and II were associated with 7.30-fold (HR:7.30, 95% CI:(3.11-17.17), p<0.001) and 2.57-fold (HR:2.57, 95% CI:(1.10-6.00), p = 0.03) increases in hazard of death relative to phenotype III.
Conclusion: We identified three clinical COVID-19 phenotypes, reflecting patient populations with different comorbidities, complications, and clinical outcomes. Future research is needed to determine the utility of these phenotypes in clinical practice and trial design.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Update of
-
Characterizing COVID-19 Clinical Phenotypes and Associated Comorbidities and Complication Profiles.medRxiv [Preprint]. 2020 Sep 14:2020.09.12.20193391. doi: 10.1101/2020.09.12.20193391. medRxiv. 2020. Update in: PLoS One. 2021 Mar 31;16(3):e0248956. doi: 10.1371/journal.pone.0248956. PMID: 32995813 Free PMC article. Updated. Preprint.
References
-
- Wu Z, McGoogan JM, (2020) Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA - PubMed
-
- Group RC, Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, et al. (2020) Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. The New England journal of medicine
-
- Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC, (2020) Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
