

Decongestion discriminates risk for one-year mortality in patients with improving renal function in acute heart failure
- PMID: 33788989
- PMCID: PMC11500646
- DOI: 10.1002/ejhf.2179
Decongestion discriminates risk for one-year mortality in patients with improving renal function in acute heart failure
Abstract
Aims: Improving renal function (IRF) is paradoxically associated with worse outcomes in acute heart failure (AHF), but outcomes may differ based on response to decongestion. We explored if the relationship of IRF with mortality in hospitalized AHF patients differs based on successful decongestion.
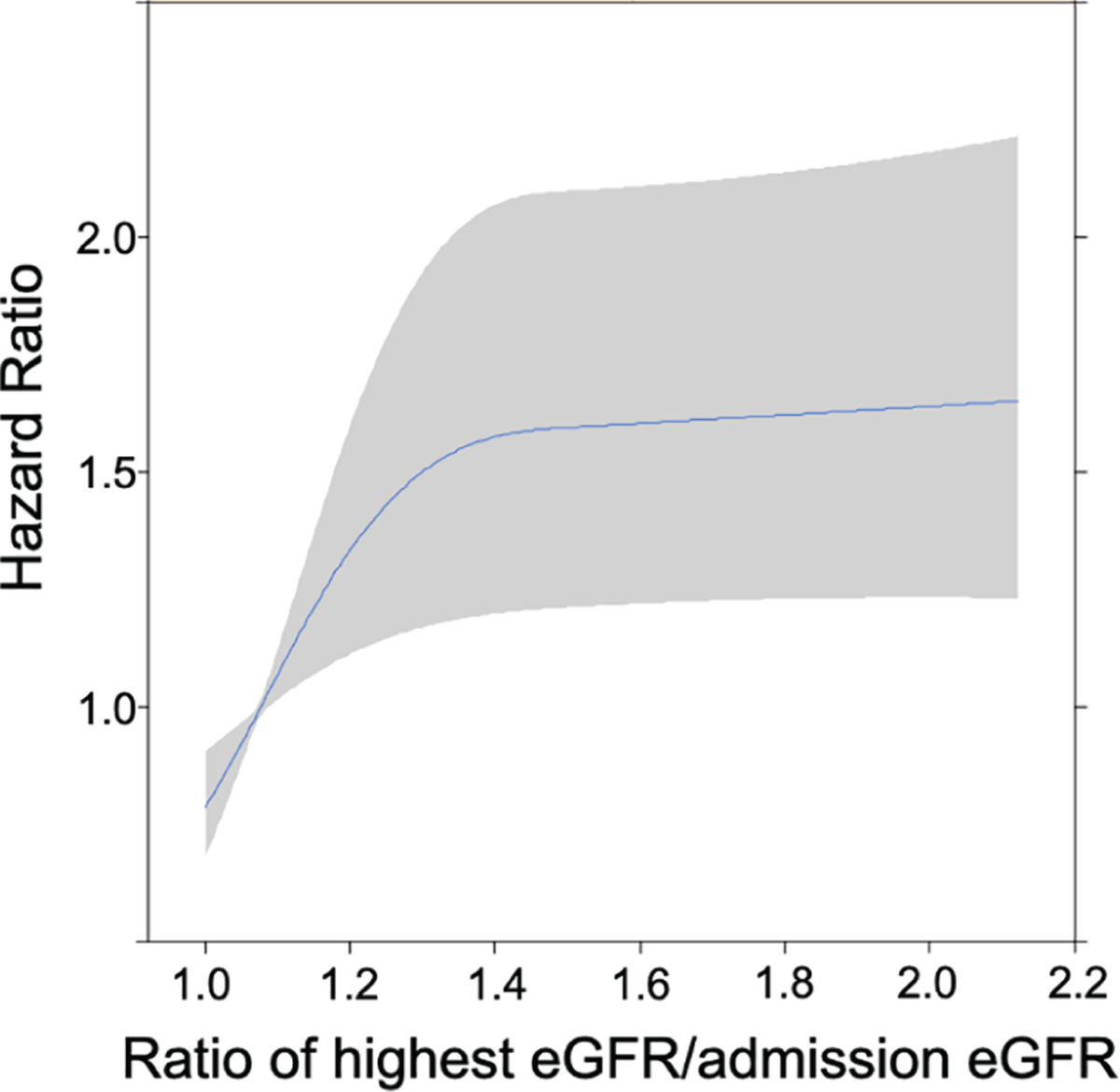
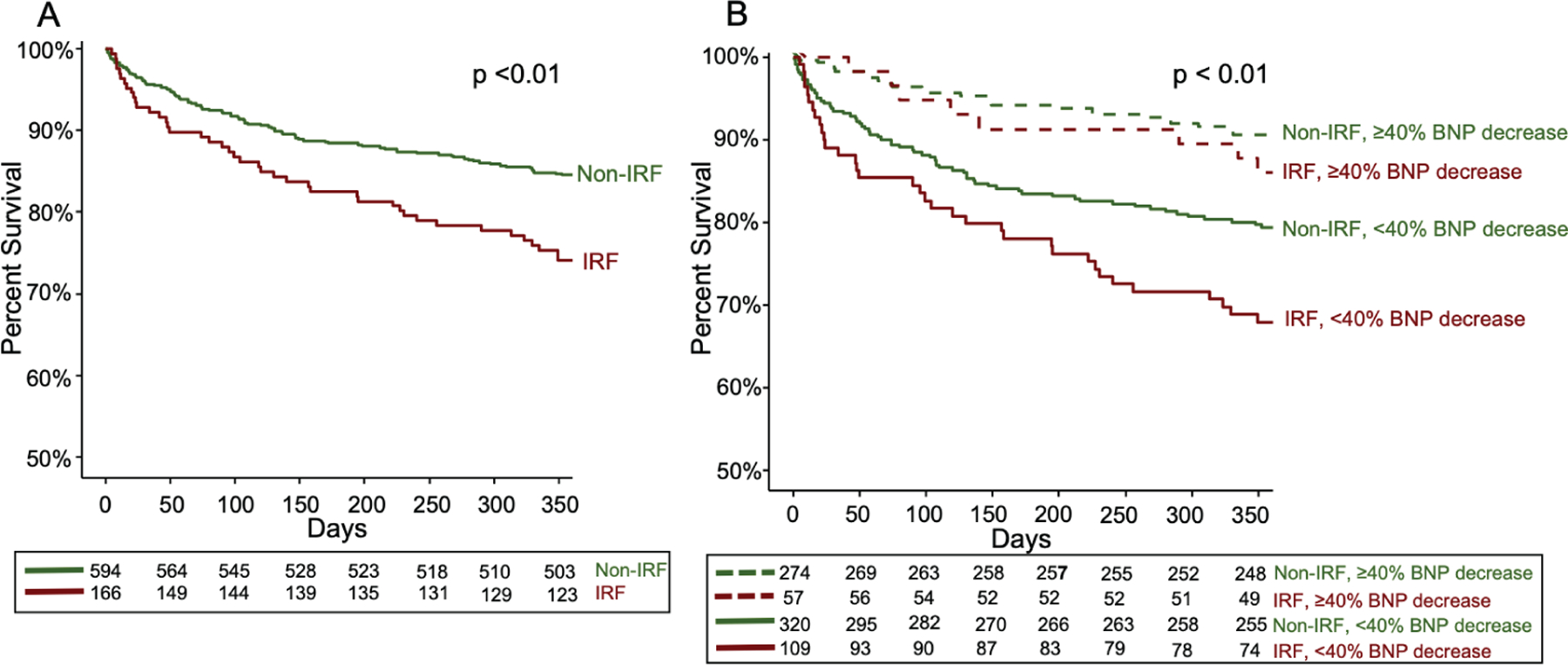
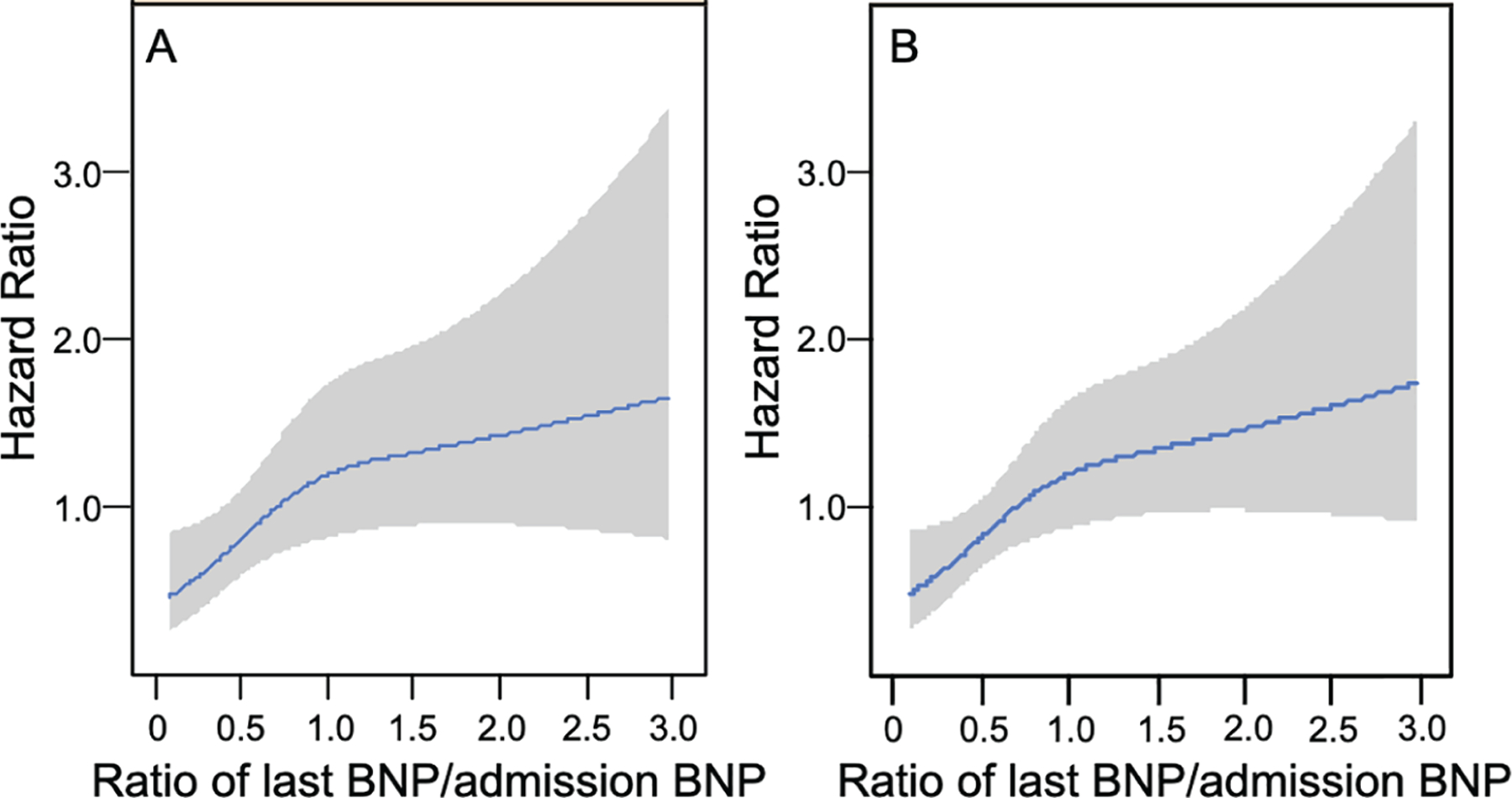
Methods and results: We evaluated 760 AHF patients from AKINESIS for the relationship between IRF, change in B-type natriuretic peptide (BNP), and 1-year mortality. IRF was defined as a ≥20% increase in estimated glomerular filtration rate (eGFR) relative to admission. Adequate decongestion was defined as a ≥40% decrease in last measured BNP relative to admission. IRF occurred in 22% of patients who had a mean age of 69 years, 58% were men, 72% were white, and median admission eGFR was 49 mL/min/1.73 m2 . IRF patients had more severe heart failure reflected by lower admission eGFR, higher blood urea nitrogen, lower systolic blood pressure, lower sodium, and higher use of inotropes. IRF patients had higher 1-year mortality (25%) than non-IRF patients (15%) (P < 0.01). However, this relationship differed by BNP trajectory (P-interaction = 0.03). When stratified by BNP change, non-IRF patients and IRF patients with decreasing BNP had lower 1-year mortality than either non-IRF and IRF patients without decreasing BNP. However, in multivariate analysis, IRF was not associated with mortality [adjusted hazard ratio (HR) 1.0, 95% confidence interval (CI) 0.7-1.5] while BNP was (adjusted HR 0.5, 95% CI 0.3-0.7). When IRF was evaluated as transiently occurring or persisting at discharge, again only BNP change was significantly associated with mortality.
Conclusion: Improving renal function is associated with mortality in AHF but not independent of other variables and congestion status. Achieving adequate decongestion, as reflected by lower BNP, in AHF is more strongly associated with mortality than IRF.
Keywords: Acute heart failure; B-type natriuretic peptide; Congestion; Kidney function; Prognosis.
© 2021 European Society of Cardiology.
Conflict of interest statement
Figures
Comment in
-
Improving renal function during diuresis: useful information or just noise?Eur J Heart Fail. 2021 Jul;23(7):1131-1133. doi: 10.1002/ejhf.2267. Epub 2021 Jun 21. Eur J Heart Fail. 2021. PMID: 34117684 No abstract available.
References
-
- Ronco C, McCullough P, Anker SD, Anand I, Aspromonte N, Bagshaw SM, Bellomo R, Berl T, Bobek I, Cruz DN, Daliento L, Davenport A, Haapio M, Hillege H, House AA, Katz N, Maisel A, Mankad S, Zanco P, Mebazaa A, Palazzuoli A, Ronco F, Shaw A, Sheinfeld G, Soni S, Vescovo G, Zamperetti N, Ponikowski P; Acute Dialysis Quality Initiative (ADQI) Consensus Group . Cardio-renal syndromes: report from the consensus conference of the Acute Dialysis Quality Initiative. Eur Heart J 2010;31:703–711. - PMC - PubMed
-
- Damman K, Valente MA, Voors AA, O’Connor CM, van Veldhuisen DJ, Hillege HL. Renal impairment, worsening renal function, and outcome in patients with heart failure: an updated meta-analysis. Eur Heart J 2014;35:455–469. - PubMed
-
- Damman K, van Deursen VM, Navis G, Voors AA, van Veldhuisen DJ, Hillege HL. Increased central venous pressure is associated with impaired renal function and mortality in a broad spectrum of patients with cardiovascular disease. J Am Coll Cardiol 2009;53:582–588. - PubMed
-
- Aronson D, Abassi Z, Allon E, Burger AJ. Fluid loss, venous congestion, and worsening renal function in acute decompensated heart failure. Eur J Heart Fail 2013;15:637–643. - PubMed
-
- Felker GM, Lee KL, Bull DA, Redfield MM, Stevenson LW, Goldsmith SR, LeWinter MM, Deswal A, Rouleau JL, Ofili EO, Anstrom KJ, Hernandez AF, McNulty SE, Velazquez EJ, Kfoury AG, Chen HH, Givertz MM, Semigran MJ, Bart BA, Mascette AM, Braunwald E, O’Connor CM; NHLBI Heart Failure Clinical Research Network. Diuretic strategies in patients with acute decompensated heart failure. N Engl J Med 2011;364:797–805. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
