

Extracorporeal Membrane Oxygenation with Right Ventricular Assist Device for COVID-19 ARDS
- PMID: 33789179
- PMCID: PMC7969863
- DOI: 10.1016/j.jss.2021.03.017
Extracorporeal Membrane Oxygenation with Right Ventricular Assist Device for COVID-19 ARDS
Abstract
Background: Right ventricular failure is an underrecognized consequence of COVID-19 pneumonia. Those with severe disease are treated with extracorporeal membrane oxygenation (ECMO) but with poor outcomes. Concomitant right ventricular assist device (RVAD) may be beneficial.
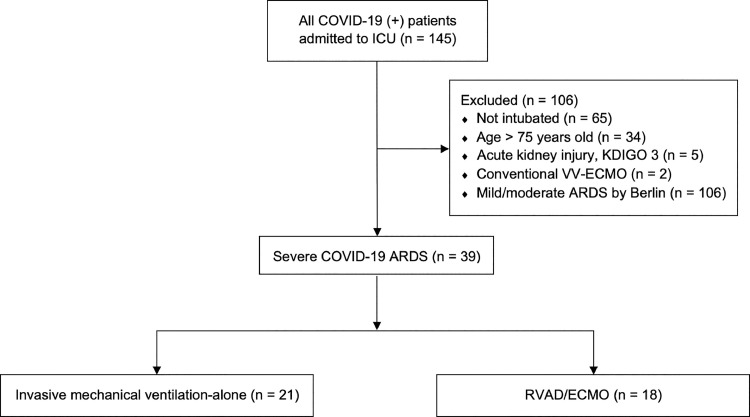
Methods: A retrospective analysis of intensive care unit patients admitted with COVID-19 ARDS (Acute Respiratory Distress Syndrome) was performed. Nonintubated patients, those with acute kidney injury, and age > 75 were excluded. Patients who underwent RVAD/ECMO support were compared with those managed via invasive mechanical ventilation (IMV) alone. The primary outcome was in-hospital mortality. Secondary outcomes included 30-d mortality, acute kidney injury, length of ICU stay, and duration of mechanical ventilation.
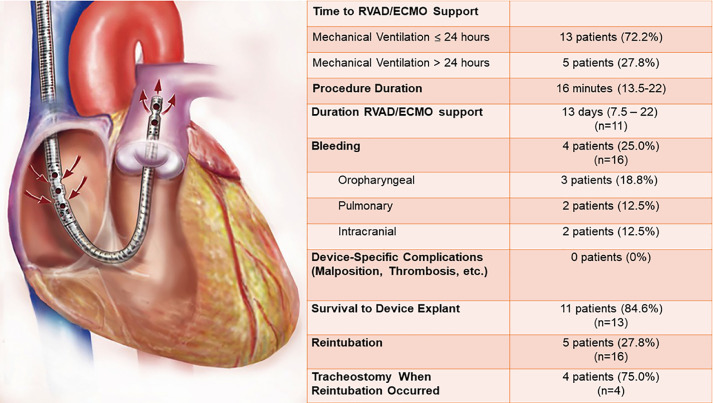
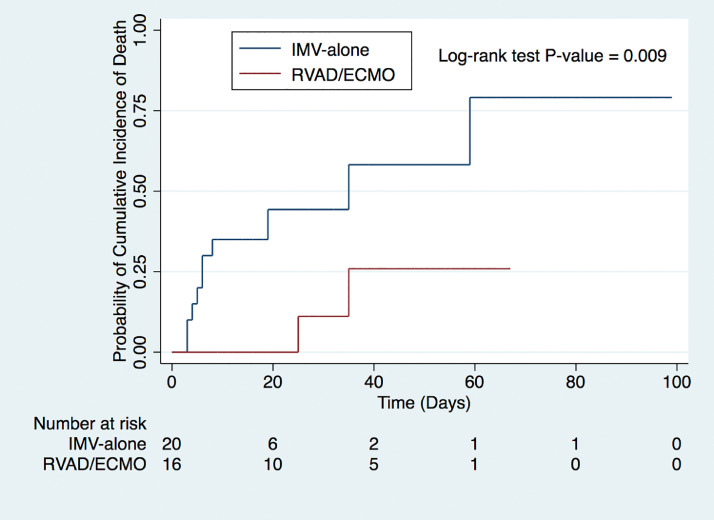
Results: A total of 145 patients were admitted to the ICU with COVID-19. Thirty-nine patients met inclusion criteria. Of these, 21 received IMV, and 18 received RVAD/ECMO. In-hospital (52.4 versus 11.1%, P = 0.008) and 30-d mortality (42.9 versus 5.6%, P= 0.011) were significantly lower in patients treated with RVAD/ECMO. Acute kidney injury occurred in 15 (71.4%) patients in the IMV group and zero RVAD/ECMO patients (P< 0.001). ICU (11.5 versus 21 d, P= 0.067) and hospital (14 versus 25.5 d, P = 0.054) length of stay were not significantly different. There were no RVAD/ECMO device complications. The duration of mechanical ventilation was not significantly different (10 versus 5 d, P = 0.44).
Conclusions: RVAD support at the time of ECMO initiation resulted in the no secondary end-organ damage and higher in-hospital and 30-d survival versus IMV in specially selected patients with severe COVID-19 ARDS. Management of severe COVID-19 ARDS should prioritize right ventricular support.
Keywords: Acute respiratory distress syndrome; COVID-19; Extracorporeal membrane oxygenation; Right ventricular assist device.
Copyright © 2021. Published by Elsevier Inc.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
