

Platelets, immune cells and the coagulation cascade; friend or foe of the circulating tumour cell?
- PMID: 33789677
- PMCID: PMC8011144
- DOI: 10.1186/s12943-021-01347-1
Platelets, immune cells and the coagulation cascade; friend or foe of the circulating tumour cell?
Abstract
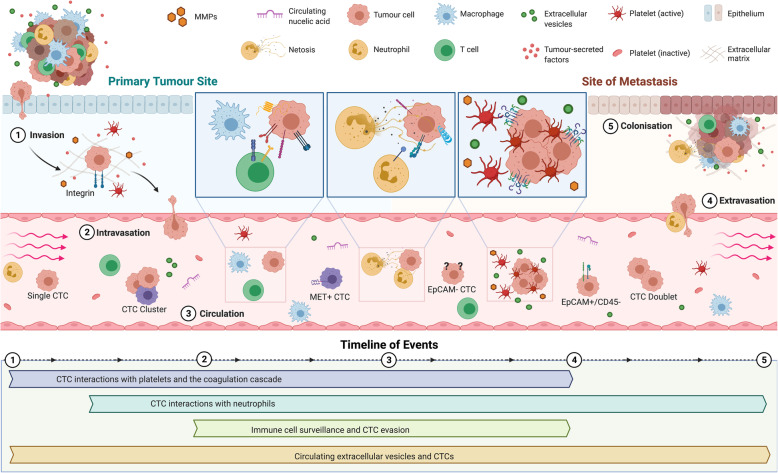
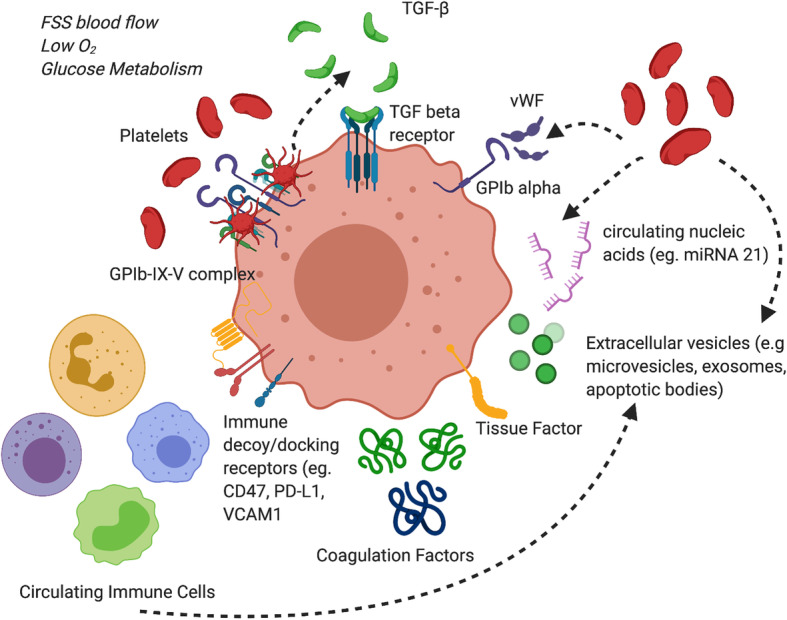
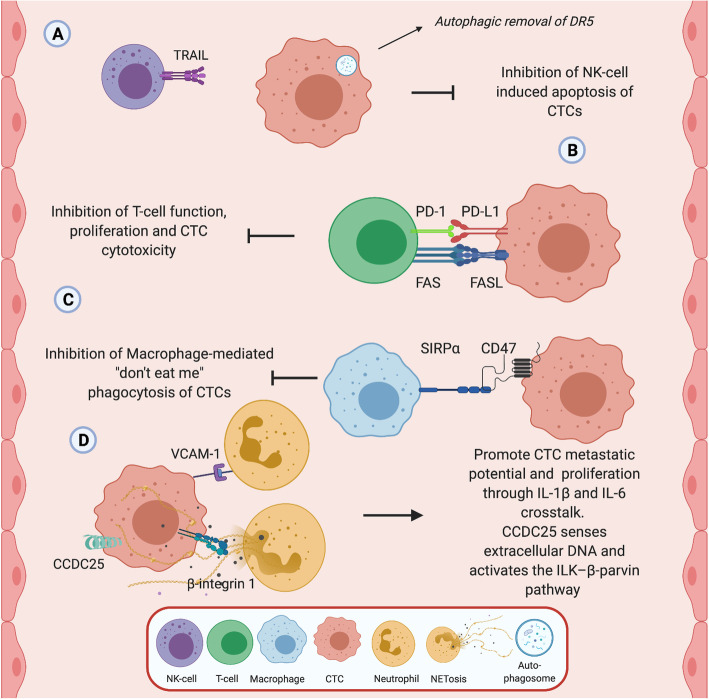
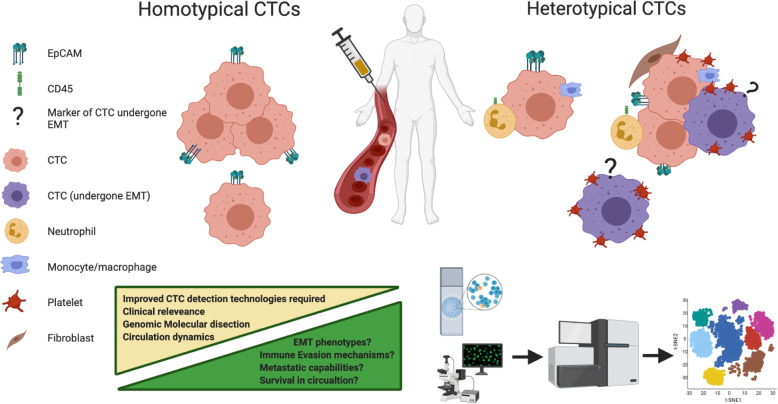
Cancer cells that transit from primary tumours into the circulatory system are known as circulating tumour cells (CTCs). These cancer cells have unique phenotypic and genotypic characteristics which allow them to survive within the circulation, subsequently extravasate and metastasise. CTCs have emerged as a useful diagnostic tool using "liquid biopsies" to report on the metastatic potential of cancers. However, CTCs by their nature interact with components of the blood circulatory system on a constant basis, influencing both their physical and morphological characteristics as well as metastatic capabilities. These properties and the associated molecular profile may provide critical diagnostic and prognostic capabilities in the clinic. Platelets interact with CTCs within minutes of their dissemination and are crucial in the formation of the initial metastatic niche. Platelets and coagulation proteins also alter the fate of a CTC by influencing EMT, promoting pro-survival signalling and aiding in evading immune cell destruction. CTCs have the capacity to directly hijack immune cells and utilise them to aid in CTC metastatic seeding processes. The disruption of CTC clusters may also offer a strategy for the treatment of advance staged cancers. Therapeutic disruption of these heterotypical interactions as well as direct CTC targeting hold great promise, especially with the advent of new immunotherapies and personalised medicines. Understanding the molecular role that platelets, immune cells and the coagulation cascade play in CTC biology will allow us to identify and characterise the most clinically relevant CTCs from patients. This will subsequently advance the clinical utility of CTCs in cancer diagnosis/prognosis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
