

Trends in reasons for emergency calls during the COVID-19 crisis in the department of Gironde, France using artificial neural network for natural language classification
- PMID: 33789721
- PMCID: PMC8011068
- DOI: 10.1186/s13049-021-00862-w
Trends in reasons for emergency calls during the COVID-19 crisis in the department of Gironde, France using artificial neural network for natural language classification
Abstract
Objectives: During periods such as the COVID-19 crisis, there is a need for responsive public health surveillance indicators in order to monitor both the epidemic growth and potential public health consequences of preventative measures such as lockdown. We assessed whether the automatic classification of the content of calls to emergency medical communication centers could provide relevant and responsive indicators.
Methods: We retrieved all 796,209 free-text call reports from the emergency medical communication center of the Gironde department, France, between 2018 and 2020. We trained a natural language processing neural network model with a mixed unsupervised/supervised method to classify all reasons for calls in 2020. Validation and parameter adjustment were performed using a sample of 39,907 manually-coded free-text reports.
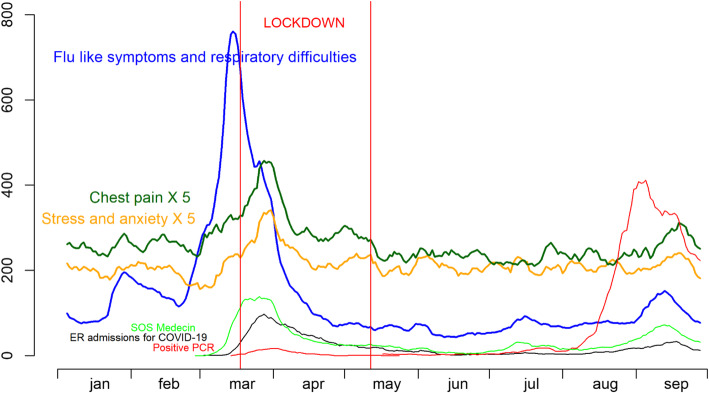
Results: The number of daily calls for flu-like symptoms began to increase from February 21, 2020 and reached an unprecedented level by February 28, 2020 and peaked on March 14, 2020, 3 days before lockdown. It was strongly correlated with daily emergency room admissions, with a delay of 14 days. Calls for chest pain and stress and anxiety, peaked 12 days later. Calls for malaises with loss of consciousness, non-voluntary injuries and alcohol intoxications sharply decreased, starting one month before lockdown. No noticeable trends in relation to lockdown was found for other groups of reasons including gastroenteritis and abdominal pain, stroke, suicide and self-harm, pregnancy and delivery problems.
Discussion: The first wave of the COVID-19 crisis came along with increased levels of stress and anxiety but no increase in alcohol intoxication and violence. As expected, call related to road traffic crashes sharply decreased. The sharp decrease in the number of calls for malaise was more surprising.
Conclusion: The content of calls to emergency medical communication centers is an efficient epidemiological surveillance data source that provides insights into the societal upheavals induced by a health crisis. The use of an automatic classification system using artificial intelligence makes it possible to free itself from the context that could influence a human coder, especially in a crisis situation. The COVID-19 crisis and/or lockdown induced deep modifications in the population health profile.
Keywords: COVID-19; Emergency medical communication centers; Lockdown; Public health.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- WHO. Coronavirus (COVID-19) events as they happen. https://www.who.int/emergencies/diseases/novel-coronavirus-2019. (Accessed Nov 1, 2020) (2020).
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
