

Case Report: Acute Thrombotic Angiopathy of Atrial Appendage Epicardial Veins: A Seemingly Innocuous Finding Portending a Fatal Outcome
- PMID: 33791344
- PMCID: PMC8006332
- DOI: 10.3389/fcvm.2021.621632
Case Report: Acute Thrombotic Angiopathy of Atrial Appendage Epicardial Veins: A Seemingly Innocuous Finding Portending a Fatal Outcome
Abstract
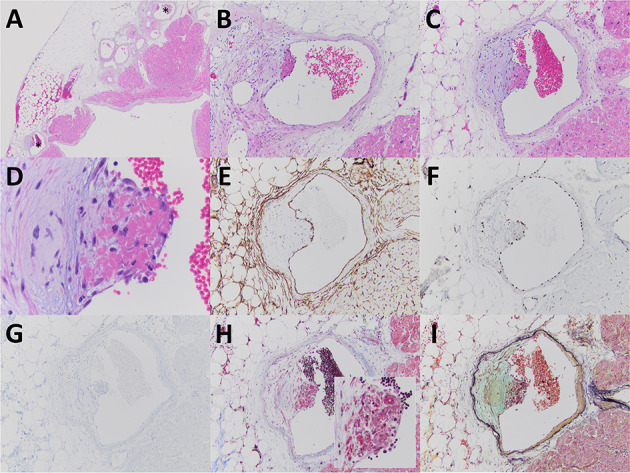
Thrombotic angiopathy is a pathologic description to describe endothelial injury, and with sufficient and sustained injury can lead to exposure of underlying tissue factor and the deposition of associated fibrin material. We present briefly a case of an 87-year-old woman with mitral valve regurgitation and atrial fibrillation undergoing mitral valve annuloplasty, Cox-maze procedure, and excision of the left atrial appendage. Pathologic examination of the excised atrial appendage revealed commonly encountered cardiomyocyte hypertrophy and endocardial fibroelastosis, however also showed a non-occlusive, acute thrombotic angiopathy involving epicardial veins. The surgical and immediate post-operative course was unremarkable; however, 3 weeks after discharge, the patient would develop a fatal pulmonary embolism. While fibrin thrombosis developing within the atrial appendage chamber is a recognized concern in the setting of atrial fibrillation, the significance of an acute thrombotic angiopathy involving epicardial veins of the atrial appendage is less clear although in the presented case was the sole potential harbinger of a subsequent fatal thrombotic event.
Keywords: acute thrombotic angiopathy; atrial appendage; atrial fibrillation; pulmonary embolism; thrombosis.
Copyright © 2021 Pichler Sekulic and Sekulic.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Castonguay MC, Wang Y, Gerhart JL, Miller DV, Stulak JM, Edwards WD, et al. Surgical pathology of atrial appendages removed during the cox-maze procedure: a review of 86 cases (2004 to 2005) with implications for prognosis. Am J Surg Pathol. (2013) 37:890–7. 10.1097/PAS.0b013e31827e180b - DOI - PubMed
-
- American College of Cardiology Foundation, American Heart Association, European Society of Cardiology, Heart Rhythm Society. Wann LS, Curtis AB, et al. Management of patients with atrial fibrillation (compilation of 2006 ACCF/AHA/ESC and 2011 ACCF/AHA/HRS recommendations): a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. Circulation. (2013) 127:1916–26. 10.1161/CIR.0b013e318290826d - DOI - PubMed
-
- Lopez JA, Ross RS, Fishbein MC, Siegel RJ. Nonbacterial thrombotic endocarditis: a review. Am Heart J. (1987) 113:773–84. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources