

Implementation of Multimodality Neurologic Monitoring Reporting in Pediatric Traumatic Brain Injury Management
- PMID: 33791948
- PMCID: PMC8012079
- DOI: 10.1007/s12028-021-01190-8
Implementation of Multimodality Neurologic Monitoring Reporting in Pediatric Traumatic Brain Injury Management
Abstract
Background/objective: Multimodality neurologic monitoring (MMM) is an emerging technique for management of traumatic brain injury (TBI). An increasing array of MMM-derived biomarkers now exist that are associated with injury severity and functional outcomes after TBI. A standardized MMM reporting process has not been well described, and a paucity of evidence exists relating MMM reporting in TBI management with functional outcomes or adverse events.
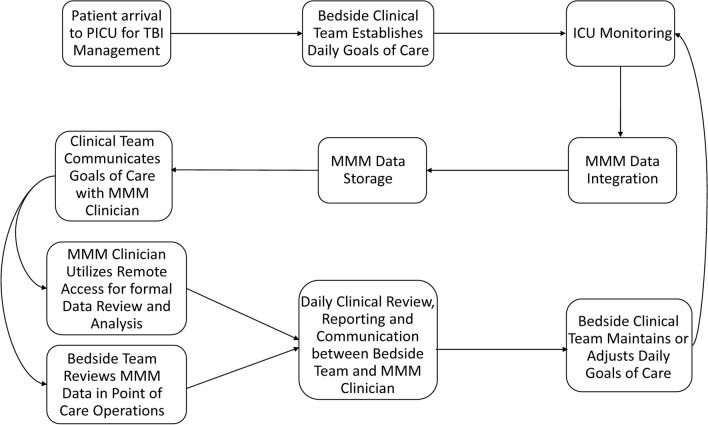
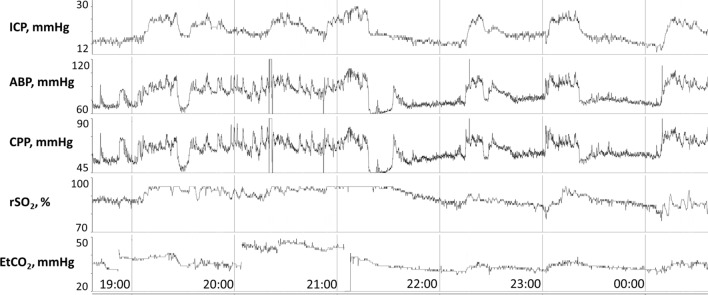
Methods: Prospective implementation of standardized MMM reporting at a single pediatric intensive care unit (PICU) is described that included monitoring of intracranial pressure (ICP), cerebral oxygenation and electroencephalography (EEG). The incidence of clinical decisions made using MMM reporting is described, including timing of neuroimaging, ICP monitoring discontinuation, use of paralytic, hyperosmolar and pentobarbital therapies, neurosurgical interventions, ventilator and CPP adjustments and neurologic prognostication discussions. Retrospective analysis was performed on the association of MMM reporting with initial Glasgow Coma Scale (GCS) and Pediatric Risk of Mortality III (PRISM III) scores, duration of total hospitalization and PICU hospitalization, duration of mechanical ventilation and invasive ICP monitoring, inpatient complications, time with ICP > 20 mmHg, time with cerebral perfusion pressure (CPP) < 40 mmHg and 12-month Glasgow Outcome Scale-Extended Pediatrics (GOSE-Peds) scores. Association of outcomes with MMM reporting was investigated using the Wilcoxon rank-sum test or Fisher's exact test, as appropriate.
Results: Eighty-five children with TBI underwent MMM over 6 years, among which 18 underwent daily MMM reporting over a 21-month period. Clinical decision-making influenced by MMM reporting included timing of neuroimaging (100.0%), ICP monitoring discontinuation (100.0%), timing of extubation trials of surviving patients (100.0%), body repositioning (11.1%), paralytic therapy (16.7%), hyperosmolar therapy (22.2%), pentobarbital therapy (33.3%), provocative cerebral autoregulation testing (16.7%), adjustments in CPP thresholds (16.7%), adjustments in PaCO2 thresholds (11.1%), neurosurgical interventions (16.7%) and neurologic prognostication discussions (11.1%). The implementation of MMM reporting was associated with a reduction in ICP monitoring duration (p = 0.0017) and mechanical ventilator duration (p = 0.0018). No significant differences were observed in initial GCS or PRISM III scores, total hospitalization length, PICU hospitalization length, total complications, time with ICP > 20 mmHg, time with CPP < 40 mmHg, use of tier 2 therapy, or 12-month GOS-E Peds scores.
Conclusion: Implementation of MMM reporting in pediatric TBI management is feasible and can be impactful in tailoring clinical decisions. Prospective work is needed to understand the impact of MMM and MMM reporting systems on functional outcomes and clinical care efficacy.
Keywords: Hospital Complications; Multimodal Neurologic Monitoring; Pediatric Neurocritical Care; Quality Improvement; Traumatic Brain Injury.
© 2021. Springer Science+Business Media, LLC, part of Springer Nature and Neurocritical Care Society.
Conflict of interest statement
Dr. Appavu reports research funding from the United States Department of Defense Congressionally Directed Medical Research Programs Epilepsy Research Program in relation to this work. He also reports a completed research grant from Moberg ICU Solutions as well as a research grant from the American Heart Association, outside of the submitted work. All other co-authors have no relevant conflicts of interest to disclose.
Figures
Comment in
-
Complex Approaches for a Complex Organ.Neurocrit Care. 2021 Aug;35(1):1-2. doi: 10.1007/s12028-021-01231-2. Epub 2021 Apr 30. Neurocrit Care. 2021. PMID: 33929706 No abstract available.
References
-
- Rivera-Lara L, Puttgen HA. Multimodality monitoring in the neurocritical care unit. Continuum (Minneap Minn). 2018;24(6):1776–1788. - PubMed
-
- Le Roux P, Menon DK, Citerio G, et al (2014) Consensus summary statement of the International Multidisciplinary Consensus Conference on Multimodality Monitoring in Neurocritical Care: a statement for healthcare professionals from the Neurocritical Care Society and the European Society of Intensive Care Medicine. Intensive Care Med. 40(9); 1189–1209. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
