

Ultrasound to identify systemic lupus erythematosus patients with musculoskeletal symptoms who respond best to therapy: the US Evaluation For mUsculoskeletal Lupus longitudinal multicentre study
- PMID: 33792659
- PMCID: PMC8566203
- DOI: 10.1093/rheumatology/keab288
Ultrasound to identify systemic lupus erythematosus patients with musculoskeletal symptoms who respond best to therapy: the US Evaluation For mUsculoskeletal Lupus longitudinal multicentre study
Abstract
Objectives: To determine whether SLE patients with inflammatory joint symptoms and US synovitis/tenosyovitis achieve better clinical responses to glucocorticoids compared with patients with normal scans. Secondary objectives included identification of clinical features predicting US synovitis/tenosynovitis.
Methods: In a longitudinal multicentre study, SLE patients with physician-diagnosed inflammatory joint pain received intramuscular methylprednisolone 120 mg once. Clinical assessments, patient-reported outcomes and bilateral hand/wrist USs were collected at 0, 2 and 6 weeks. The primary outcome (determined via internal pilot) was the early morning stiffness visual analogue scale (EMS-VAS) at 2 weeks, adjusted for baseline, comparing patients with positive (greyscale ≥2 and/or power Doppler ≥1) and negative US. Post hoc analyses excluded FM.
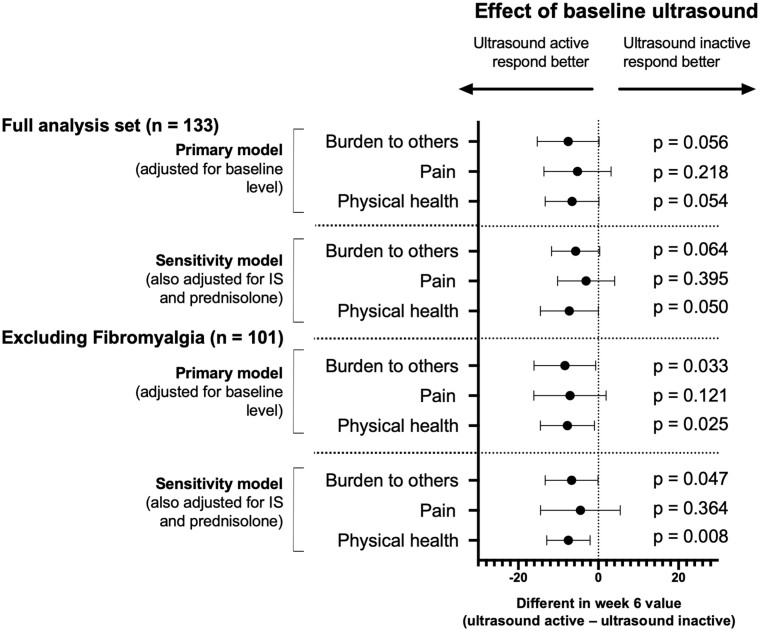
Results: Of 133 patients, 78 had a positive US. Only 53 (68%) of these had one or more swollen joint. Of 66 patients with one or more swollen joint, 20% had a negative US. A positive US was associated with joint swelling, symmetrical small joint distribution and serology. The primary endpoint was not met: in the full analysis set (N = 133) there was no difference in baseline-adjusted EMS-VAS at week 2 [-7.7 mm (95% CI -19.0, 3.5); P = 0.178]. After excluding 32 patients with FM, response was significantly better in patients with a positive US at baseline [baseline-adjusted EMS-VAS at 2 weeks -12.1 mm (95% CI -22.2, -0.1); P = 0.049]. This difference was greater when adjusted for treatment [-12.8 mm (95% CI -22, -3); P = 0.007]. BILAG and SLEDAI responses were higher in US-positive patients.
Conclusion: In SLE patients without FM, those with a positive US had a better clinical response to therapy. Imaging-detected synovitis/tenosynovitis may be considered to decide on therapy and enrich clinical trials.
Keywords: biomarkers; clinical trials and methods; outcome measures; systemic lupus erythematosus; ultrasound.
© The Author(s) 2021. Published by Oxford University Press on behalf of the British Society for Rheumatology.
Figures


References
-
- Mahmoud K, Zayat A, Vital EM.. Musculoskeletal manifestations of systemic lupus erythmatosus. Curr Opin Rheumatol 2017;29:486–92. - PubMed
-
- Pettersson S, Lovgren M, Eriksson LE. et al. An exploration of patient-reported symptoms in systemic lupus erythematosus and the relationship to health-related quality of life. Scand J Rheumatol 2012;41:383–90. - PubMed
-
- Isenberg DA, Rahman A, Allen E. et al. BILAG 2004. Development and initial validation of an updated version of the British Isles Lupus Assessment Group’s disease activity index for patients with systemic lupus erythematosus. Rheumatology (Oxford) 2005;44:902–6. - PubMed
-
- Gladman DD, Ibanez D, Urowitz MB.. Systemic lupus erythematosus disease activity index 2000. J Rheumatol 2002;29:288–91. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
