

Effects of dapagliflozin on mortality in patients with chronic kidney disease: a pre-specified analysis from the DAPA-CKD randomized controlled trial
- PMID: 33792669
- PMCID: PMC8244648
- DOI: 10.1093/eurheartj/ehab094
Effects of dapagliflozin on mortality in patients with chronic kidney disease: a pre-specified analysis from the DAPA-CKD randomized controlled trial
Abstract
Aims: Mortality rates from chronic kidney disease (CKD) have increased in the last decade. In this pre-specified analysis of the DAPA-CKD trial, we determined the effects of dapagliflozin on cardiovascular and non-cardiovascular causes of death.
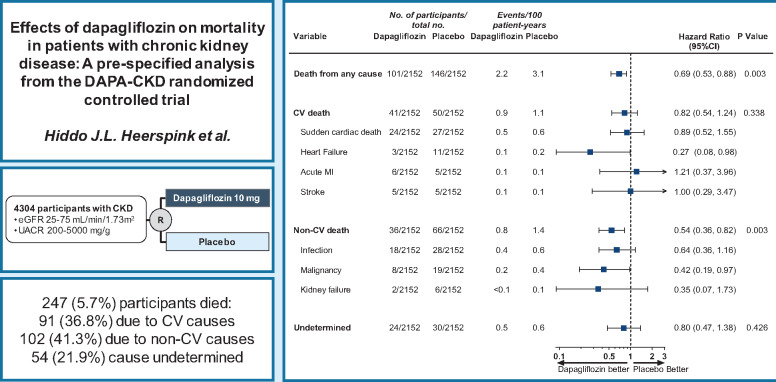
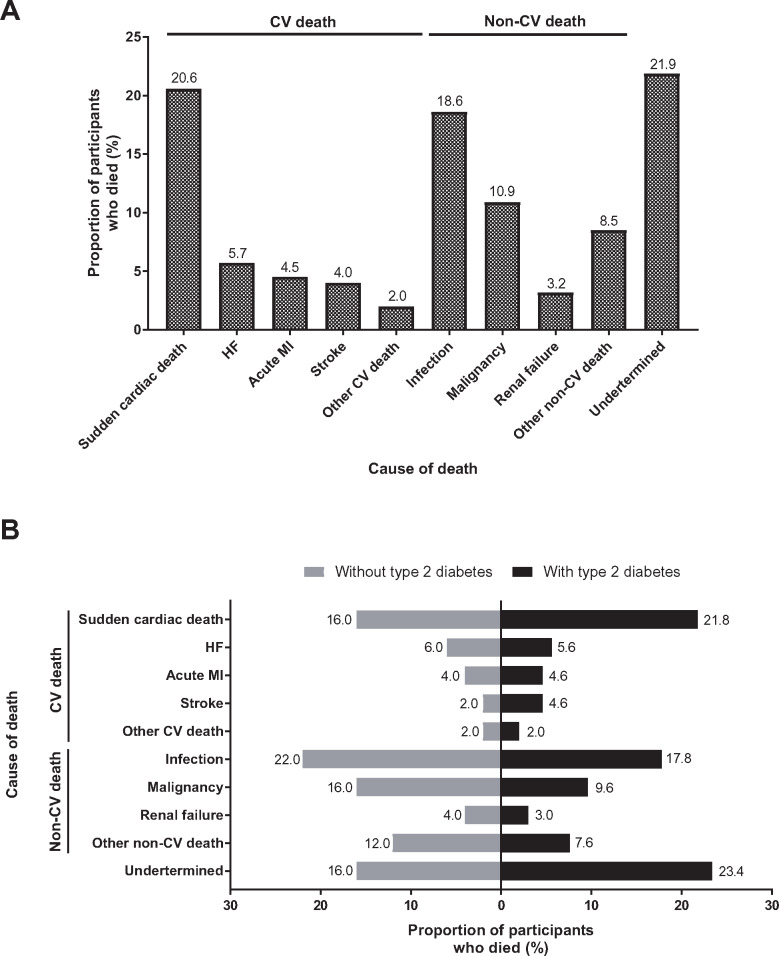
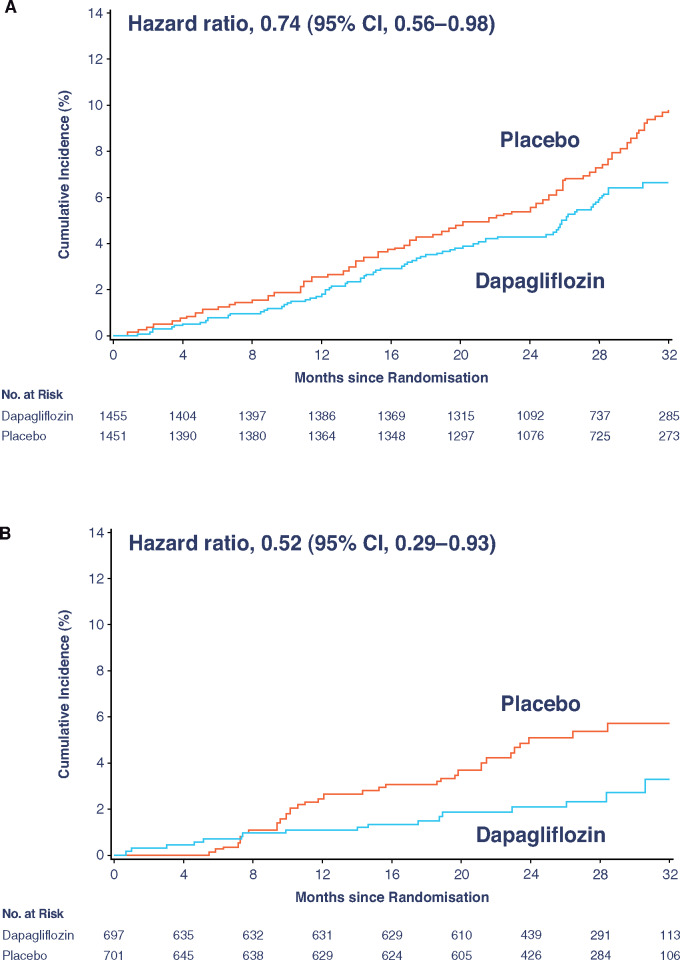
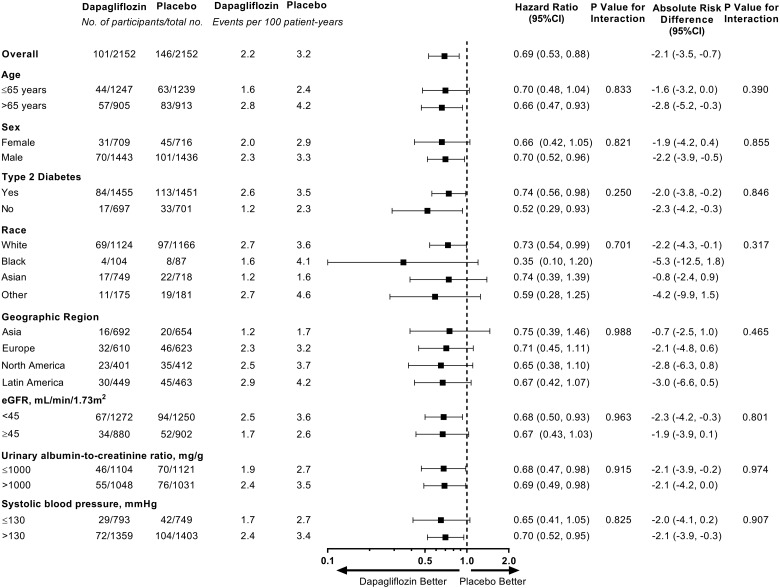
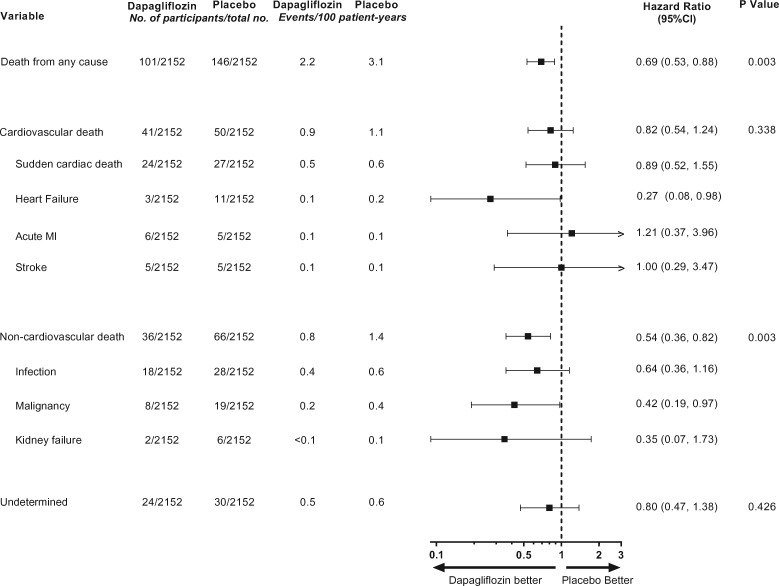
Methods and results: DAPA-CKD was an international, randomized, placebo-controlled trial with a median of 2.4 years of follow-up. Eligible participants were adult patients with CKD, defined as a urinary albumin-to-creatinine ratio (UACR) 200-5000 mg/g and an estimated glomerular filtration rate (eGFR) 25-75 mL/min/1.73 m2. All-cause mortality was a key secondary endpoint. Cardiovascular and non-cardiovascular death was adjudicated by an independent clinical events committee. The DAPA-CKD trial randomized participants to dapagliflozin 10 mg/day (n = 2152) or placebo (n = 2152). The mean age was 62 years, 33% were women, the mean eGFR was 43.1 mL/min/1.73 m2, and the median UACR was 949 mg/g. During follow-up, 247 (5.7%) patients died, of whom 91 (36.8%) died due to cardiovascular causes, 102 (41.3%) due to non-cardiovascular causes, and in 54 (21.9%) patients, the cause of death was undetermined. The relative risk reduction for all-cause mortality with dapagliflozin (31%, hazard ratio [HR] [95% confidence interval (CI)] 0.69 [0.53, 0.88]; P = 0.003) was consistent across pre-specified subgroups. The effect on all-cause mortality was driven largely by a 46% relative risk reduction of non-cardiovascular death (HR [95% CI] 0.54 [0.36, 0.82]). Deaths due to infections and malignancies were the most frequently occurring causes of non-cardiovascular deaths and were reduced with dapagliflozin vs. placebo.
Conclusion: In patients with CKD, dapagliflozin prolonged survival irrespective of baseline patient characteristics. The benefits were driven largely by reductions in non-cardiovascular death.
Keywords: Chronic kidney disease; Dapagliflozin; SGLT2 inhibitor.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Dapagliflozin, advanced chronic kidney disease, and mortality: new insights from the DAPA-CKD trial.Eur Heart J. 2021 Mar 31;42(13):1228-1230. doi: 10.1093/eurheartj/ehab092. Eur Heart J. 2021. PMID: 33792668 Free PMC article. No abstract available.
References
-
- Mosenzon O, Wiviott SD, Cahn A, Rozenberg A, Yanuv I, Goodrich EL, Murphy SA, Heerspink HJL, Zelniker TA, Dwyer JP, Bhatt DL, Leiter LA, McGuire DK, Wilding JPH, Kato ET, Gause-Nilsson IAM, Fredriksson M, Johansson PA, Langkilde AM, Sabatine MS, Raz I.. Effects of dapagliflozin on development and progression of kidney disease in patients with type 2 diabetes: an analysis from the DECLARE-TIMI 58 randomised trial. Lancet Diabetes Endocrinol 2019;7:606–617. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
