

Therapy-Induced Senescence: Opportunities to Improve Anticancer Therapy
- PMID: 33792717
- PMCID: PMC8486333
- DOI: 10.1093/jnci/djab064
Therapy-Induced Senescence: Opportunities to Improve Anticancer Therapy
Erratum in
-
Correction to: Therapy-Induced Senescence: Opportunities to Improve Anticancer Therapy.J Natl Cancer Inst. 2023 Feb 8;115(2):235. doi: 10.1093/jnci/djac225. J Natl Cancer Inst. 2023. PMID: 36519712 Free PMC article. No abstract available.
Abstract
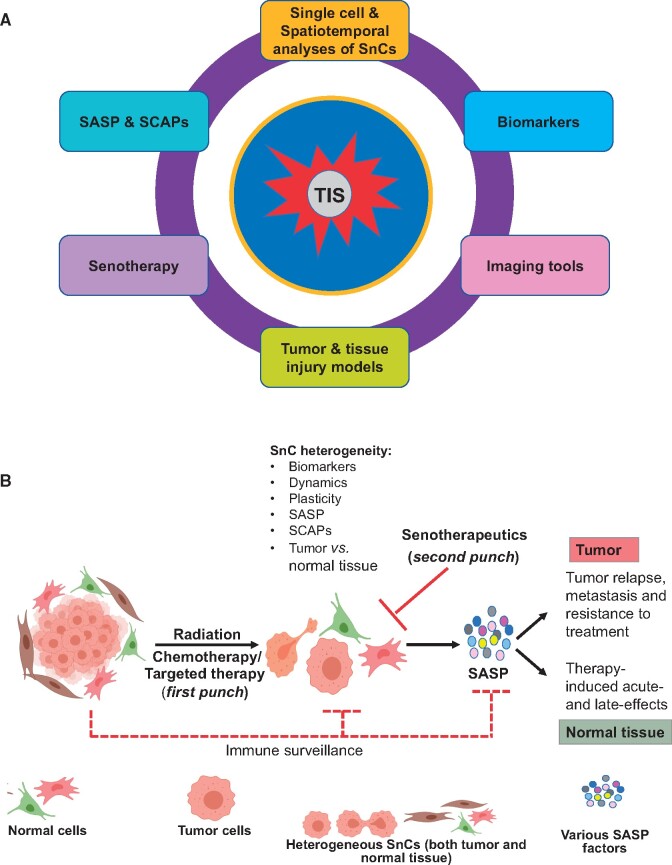
Cellular senescence is an essential tumor suppressive mechanism that prevents the propagation of oncogenically activated, genetically unstable, and/or damaged cells. Induction of tumor cell senescence is also one of the underlying mechanisms by which cancer therapies exert antitumor activity. However, an increasing body of evidence from preclinical studies demonstrates that radiation and chemotherapy cause accumulation of senescent cells (SnCs) both in tumor and normal tissue. SnCs in tumors can, paradoxically, promote tumor relapse, metastasis, and resistance to therapy, in part, through expression of the senescence-associated secretory phenotype. In addition, SnCs in normal tissue can contribute to certain radiation- and chemotherapy-induced side effects. Because of its multiple roles, cellular senescence could serve as an important target in the fight against cancer. This commentary provides a summary of the discussion at the National Cancer Institute Workshop on Radiation, Senescence, and Cancer (August 10-11, 2020, National Cancer Institute, Bethesda, MD) regarding the current status of senescence research, heterogeneity of therapy-induced senescence, current status of senotherapeutics and molecular biomarkers, a concept of "one-two punch" cancer therapy (consisting of therapeutics to induce tumor cell senescence followed by selective clearance of SnCs), and its integration with personalized adaptive tumor therapy. It also identifies key knowledge gaps and outlines future directions in this emerging field to improve treatment outcomes for cancer patients.
© The Author(s) 2021. Published by Oxford University Press.
Figures

References
-
- Munoz-Espin D, Serrano M.. Cellular senescence: from physiology to pathology. Nat Rev Mol Cell Biol. 2014;15(7):482–496. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R21 CA205660/CA/NCI NIH HHS/United States
- I01 BX002301/BX/BLRD VA/United States
- R01 CA219836/CA/NCI NIH HHS/United States
- R01 CA242003/CA/NCI NIH HHS/United States
- R01 AG065396/AG/NIA NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- R01 CA257148/CA/NCI NIH HHS/United States
- R01 CA116021/CA/NCI NIH HHS/United States
- MC_U120085810/MRC_/Medical Research Council/United Kingdom
- R37 CA222294/CA/NCI NIH HHS/United States
- R01 CA246807/CA/NCI NIH HHS/United States
- IK6 BX005225/BX/BLRD VA/United States
- R01 CA214025/CA/NCI NIH HHS/United States
- R37 AG013925/AG/NIA NIH HHS/United States
- 28647/CRUK_/Cancer Research UK/United Kingdom
- R01 CA217182/CA/NCI NIH HHS/United States
- R01 CA243326/CA/NCI NIH HHS/United States
- P30 AG013319/AG/NIA NIH HHS/United States
- R01 AG063801/AG/NIA NIH HHS/United States
- P01 AG062413/AG/NIA NIH HHS/United States
- P01 CA094060/CA/NCI NIH HHS/United States
- R01 CA164492/CA/NCI NIH HHS/United States
- P01 CA129243/CA/NCI NIH HHS/United States
- R01 CA253678/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
