

Comparison of 4-Factor Prothrombin Complex Concentrate With Frozen Plasma for Management of Hemorrhage During and After Cardiac Surgery: A Randomized Pilot Trial
- PMID: 33792729
- PMCID: PMC8017469
- DOI: 10.1001/jamanetworkopen.2021.3936
Comparison of 4-Factor Prothrombin Complex Concentrate With Frozen Plasma for Management of Hemorrhage During and After Cardiac Surgery: A Randomized Pilot Trial
Abstract
Importance: Approximately 15% of patients undergoing cardiac surgery receive frozen plasma (FP) for bleeding. Four-factor prothrombin complex concentrates (PCCs) have logistical and safety advantages over FP and may be a suitable alternative.
Objectives: To determine the proportion of patients who received PCC and then required FP, explore hemostatic effects and safety, and assess the feasibility of study procedures.
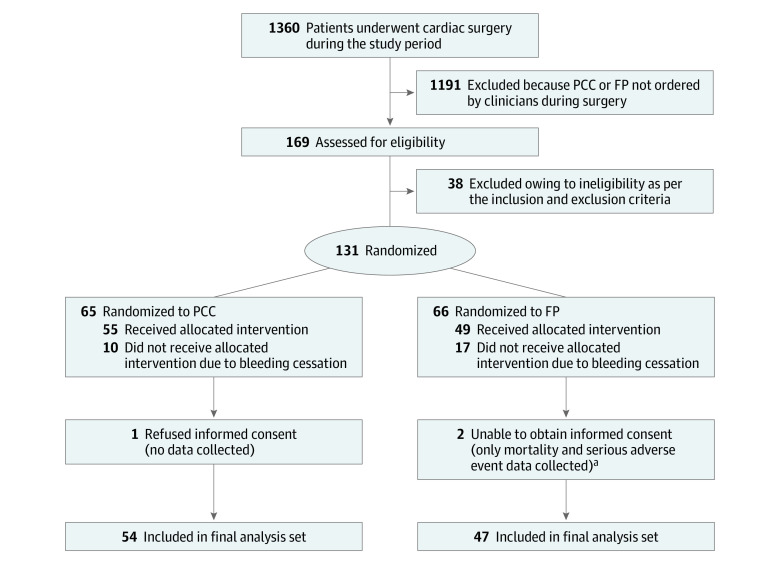
Design, setting, and participants: Parallel-group randomized pilot study conducted at 2 Canadian hospitals. Adult patients requiring coagulation factor replacement for bleeding during cardiac surgery (from September 23, 2019, to June 19, 2020; final 28-day follow-up visit, July 17, 2020). Data analysis was initiated on September 15, 2020.
Interventions: Prothrombin complex concentrate (1500 IU for patients weighing ≤60 kg and 2000 IU for patients weighing >60 kg) or FP (3 U for patients weighing ≤60 kg and 4 U for patients weighing >60 kg), repeated once as needed within 24 hours (FP used for any subsequent doses in both groups). Patients and outcome assessors were blinded to treatment allocation.
Main outcomes and measures: Hemostatic effectiveness (whether patients received any hemostatic therapies from 60 minutes to 4 and 24 hours after initiation of the intervention, amount of allogeneic blood components administered within 24 hours after start of surgery, and avoidance of red cell transfusions within 24 hours after start of surgery), protocol adherence, and adverse events. The analysis set comprised all randomized patients who had undergone cardiac surgery, received at least 1 dose of either treatment, and provided informed consent after surgery.
Results: Of 169 screened patients, 131 were randomized, and 101 were treated (54 with PCC and 47 with FP), provided consent, and were included in the analysis (median age, 64 years; interquartile range [IQR], 54-73 years; 28 [28%] were female; 82 [81%] underwent complex operations). The PCC group received a median 24.9 IU/kg (IQR, 21.8-27.0 IU/kg) of PCC (2 patients [3.7%; 95% CI, 0.4%-12.7%] required FP). The FP group received a median 12.5 mL/kg (IQR, 10.0-15.0 mL/kg) of FP (4 patients [8.5%; 95% CI, 2.4%-20.4%] required >2 doses of FP). Hemostatic therapy was not required at the 4-hour time point for 43 patients (80%) in the PCC group and for 32 patients (68%) in the FP group (P = .25) nor at the 24-hour time point for 41 patients (76%) in the PCC group and for 31 patients (66%) patients in the FP group (P = .28). The median numbers of units for 24-hour cumulative allogeneic transfusions (red blood cells, platelets, and FP) were 6.0 U (IQR, 4.0-11.0 U) in the PCC group and 14.0 U (IQR, 8.0-20.0 U) in the FP group (ratio, 0.58; 95% CI, 0.45-0.77; P < .001). After exclusion of FP administered as part of the investigational medicinal product, the median numbers of units were 6.0 U (IQR, 4.0-11.0 U) in the PCC group and 10.0 U (IQR, 6.0-16.0 U) in the FP group (ratio, 0.80; 95% CI, 0.59-1.08; P = .15). For red blood cells alone, the median numbers were 1.5 U (IQR, 0.0-4.0 U) in the PCC group and 3.0 U (IQR, 1.0-5.0 U) in the FP group (ratio, 0.69; 95% CI, 0.47-0.99; P = .05). During the first 24 hours after start of surgery, 15 patients in the PCC group (28%) and 8 patients in the FP group (17%) received no red blood cells (P = .24). Adverse event profiles were similar.
Conclusions and relevance: This randomized clinical trial found that the study protocols were feasible. Adequately powered randomized clinical trials are warranted to determine whether PCC is a suitable substitute for FP for mitigation of bleeding in cardiac surgery.
Trial registration: ClinicalTrials.gov Identifier: NCT04114643.
Conflict of interest statement
Figures
References
-
- Kremers RM, Bosch YP, Bloemen S, et al. A reduction of prothrombin conversion by cardiac surgery with cardiopulmonary bypass shifts the haemostatic balance towards bleeding. Thromb Haemost. 2016;116(3):442-451. - PubMed
-
- Ferraris VA, Brown JR, Despotis GJ, et al. ; Society of Thoracic Surgeons Blood Conservation Guideline Task Force; Society of Cardiovascular Anesthesiologists Special Task Force on Blood Transfusion; International Consortium for Evidence Based Perfusion . 2011 update to the Society of Thoracic Surgeons and the Society of Cardiovascular Anesthesiologists blood conservation clinical practice guidelines. Ann Thorac Surg. 2011;91(3):944-982. doi: 10.1016/j.athoracsur.2010.11.078 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
