

COVID-19 and the emergency presentation of colorectal cancer
- PMID: 33793063
- PMCID: PMC8250723
- DOI: 10.1111/codi.15662
COVID-19 and the emergency presentation of colorectal cancer
Abstract
Aim: The COVID-19 pandemic led to widespread disruption of colorectal cancer services during 2020. Established cancer referral pathways were modified in response to reduced diagnostic availability. The aim of this paper is to assess the impact of COVID-19 on colorectal cancer referral, presentation and stage.
Methods: This was a single centre, retrospective cohort study performed at a tertiary referral centre. Patients diagnosed and managed with colorectal adenocarcinoma between January and December 2020 were compared with patients from 2018 and 2019 in terms of demographics, mode of presentation and pathological cancer staging.
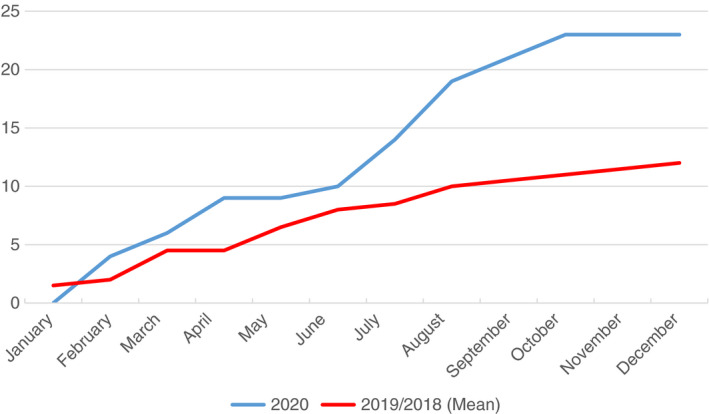
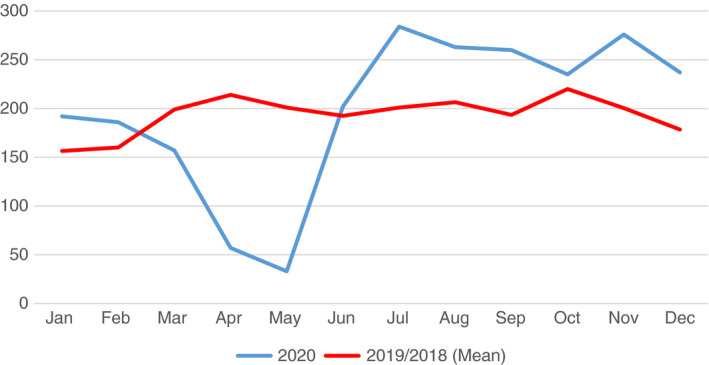
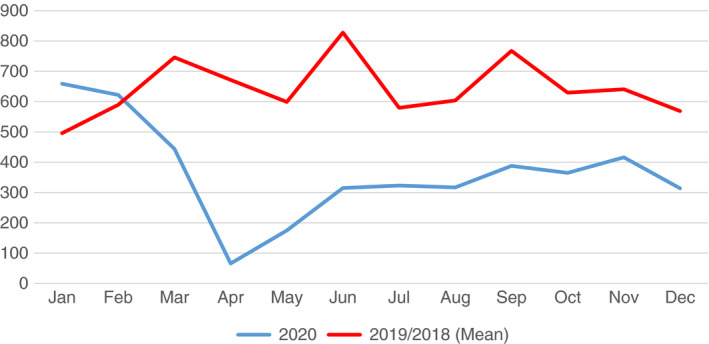
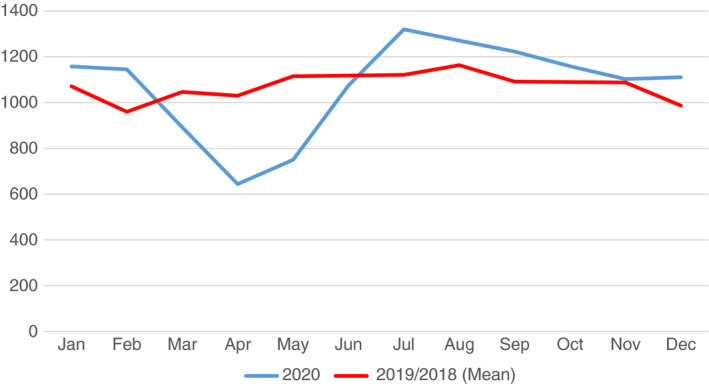
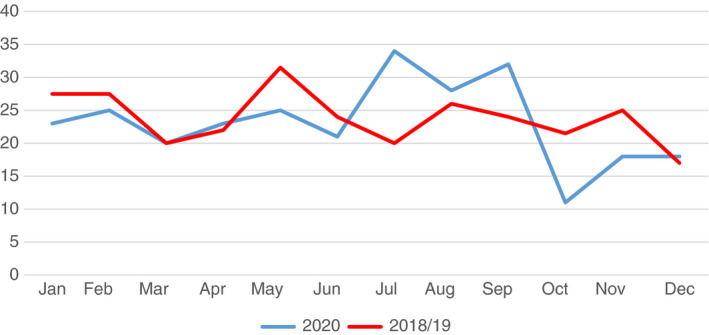
Results: In all, 272 patients were diagnosed with colorectal adenocarcinoma during 2020 compared with 282 in 2019 and 257 in 2018. Patients in all years were comparable for age, gender and tumour location (P > 0.05). There was a significant decrease in urgent suspected cancer referrals, diagnostic colonoscopy and radiological imaging performed between March and June 2020 compared with previous years. More patients presented as emergencies (P = 0.03) with increased rates of large bowel obstruction in 2020 compared with 2018-2019 (P = 0.01). The distribution of TNM grade was similar across the 3 years but more T4 cancers were diagnosed in 2020 versus 2018-2019 (P = 0.03).
Conclusion: This study demonstrates that a relatively short-term impact on the colorectal cancer referral pathway can have significant consequences on patient presentation leading to higher risk emergency presentation and surgery at a more advanced stage. It is therefore critical that efforts are made to make this pathway more robust to minimize the impact of other future adverse events and to consolidate the benefits of earlier diagnosis and treatment.
Keywords: COVID-19; cancer outcomes; colorectal cancer; coronavirus.
© 2021 The Association of Coloproctology of Great Britain and Ireland.
Conflict of interest statement
There are no relevant disclosures or conflicts of interest to declare related to this project, and no sources of funding or financial relationships.
Figures
References
-
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID‐19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323(13):1239–42. 10.1001/jama.2020.2648 [online ahead of print] - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
