

Intact parathyroid hormone levels localize causative glands in persistent or recurrent renal hyperparathyroidism: A retrospective cohort study
- PMID: 33793603
- PMCID: PMC8016254
- DOI: 10.1371/journal.pone.0248366
Intact parathyroid hormone levels localize causative glands in persistent or recurrent renal hyperparathyroidism: A retrospective cohort study
Abstract
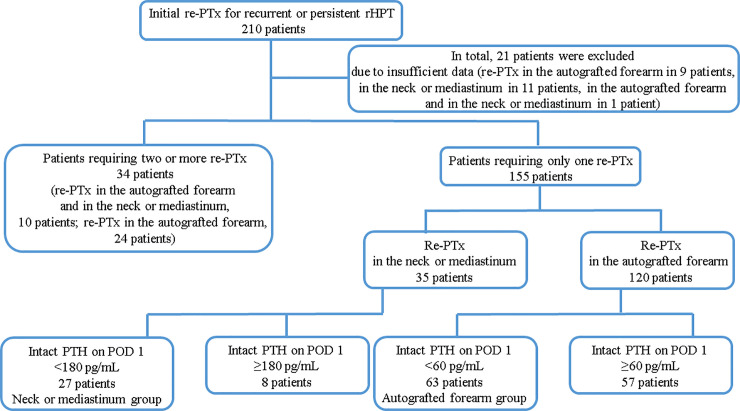
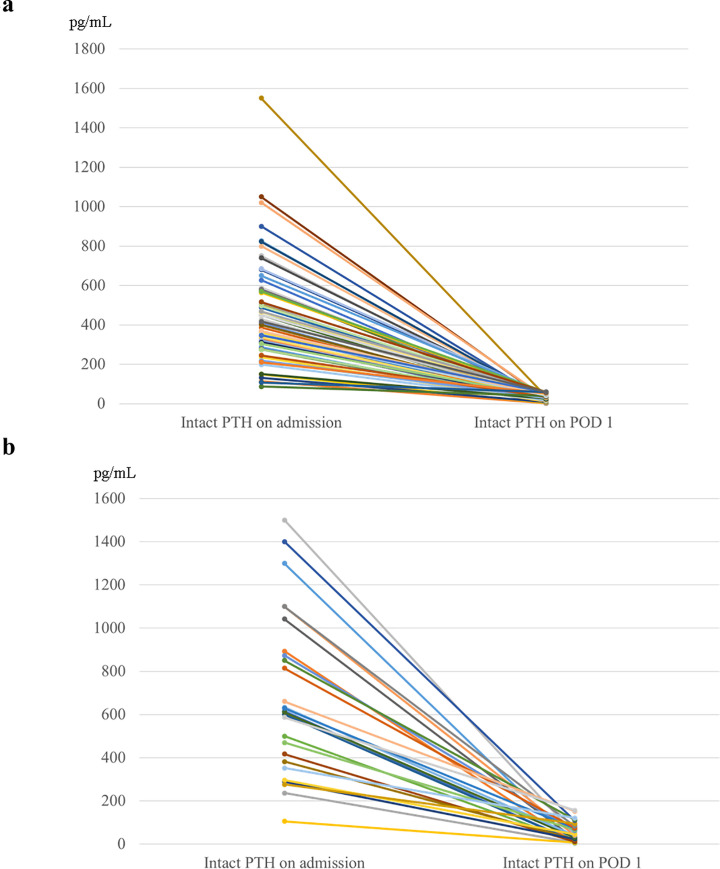
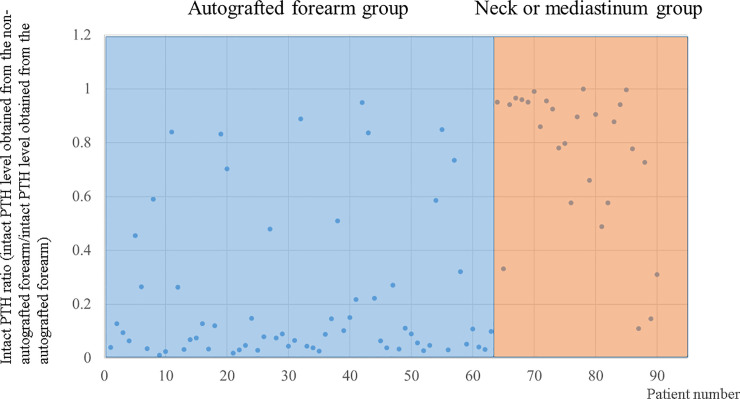
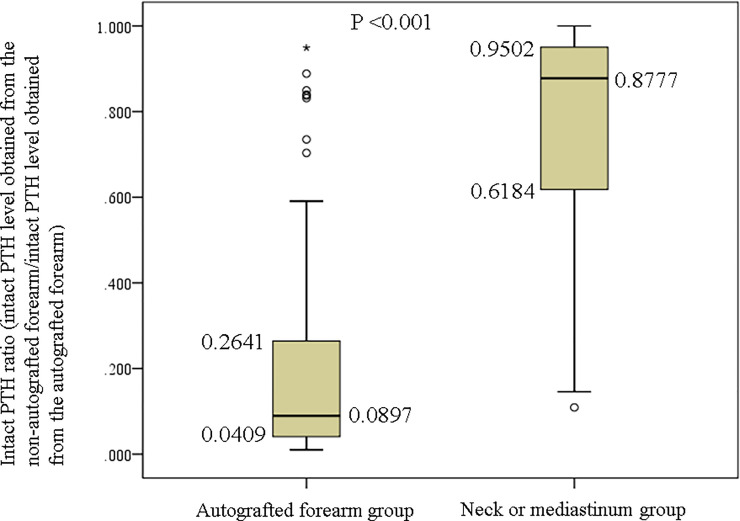
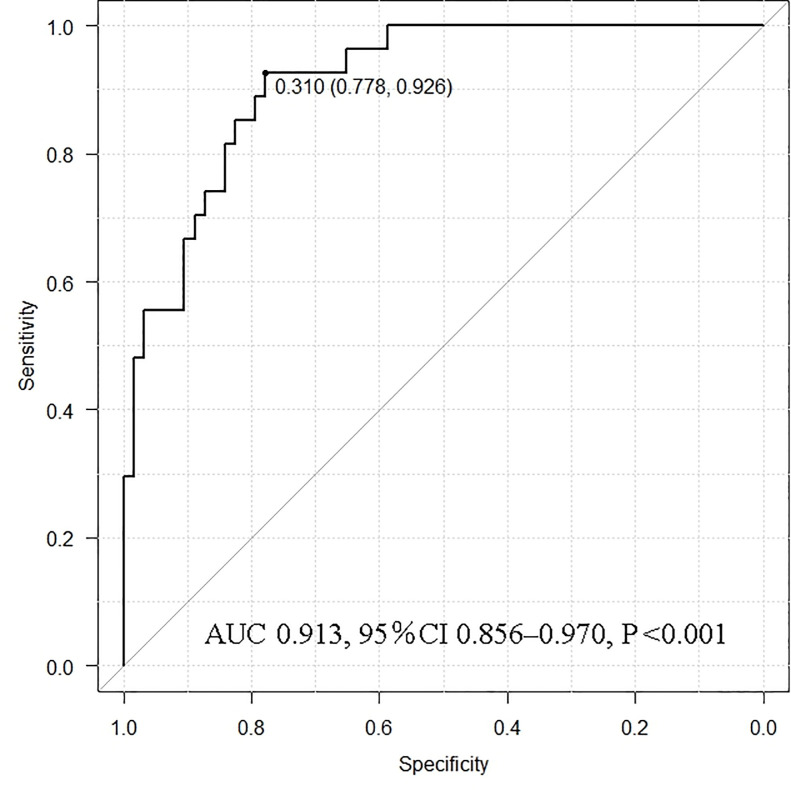
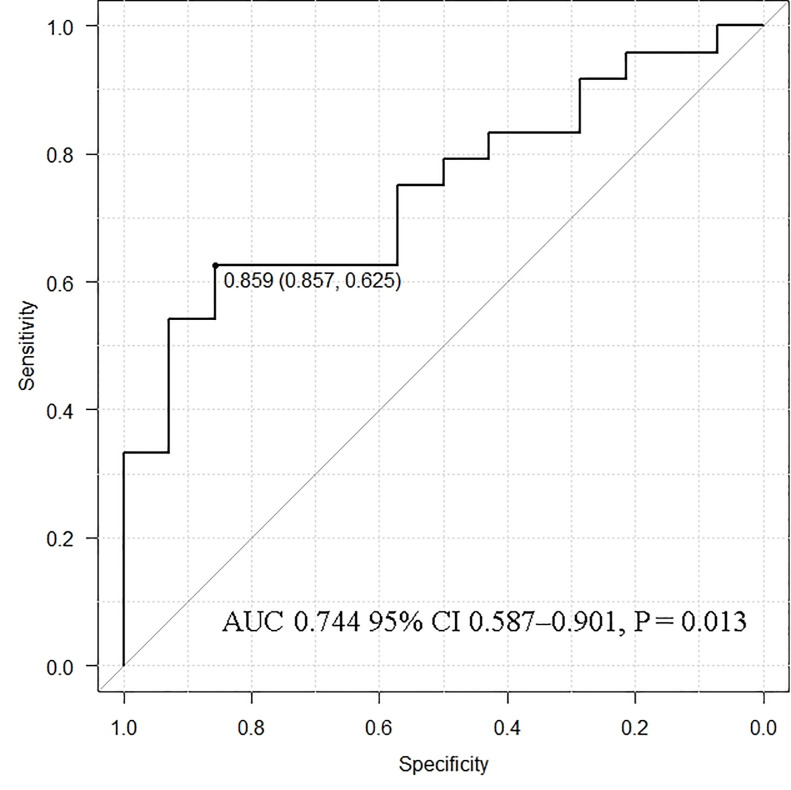
Persistent or recurrent renal hyperparathyroidism may occur after total parathyroidectomy and transcervical thymectomy with forearm autograft under continuous stimulation due to uremia. Parathyroid hormone (PTH) levels may reflect persistent or recurrent renal hyperparathyroidism because of the enlarged autografted parathyroid glands in the forearm or remnant parathyroid glands in the neck or mediastinum. Detailed imaging requires predictive localization of causative parathyroid glands. Casanova and simplified Casanova tests may be convenient. However, these methods require avascularization of the autografted forearm for >10 min with a tourniquet or Esmarch. The heavy pressure during avascularization can be incredibly painful and result in nerve damage. An easier method that minimizes the burden on patients in addition to predicting the localization of causative parathyroid glands was developed in this study. Ninety patients who underwent successful re-parathyroidectomy for persistent or recurrent renal hyperparathyroidism after parathyroidectomy between January 2000 and July 2019 were classified according to the localization of causative parathyroid glands (63 and 27 patients in the autografted forearm and the neck or mediastinum groups, respectively). Preoperatively, intact PTH levels were measured from bilateral forearm blood samples following a 5-min avascularization of the autografted forearm. Cutoff values of the intact PTH ratio (intact PTH level obtained from the non-autografted forearm before re-parathyroidectomy/intact PTH level obtained from the autografted forearm before re-parathyroidectomy) were investigated with receiver operating characteristic curves to localize the causative parathyroid glands. Intact PTH ratios of <0.310 with an area under the curve (AUC) of 0.913 (95% confidence interval [CI]: 0.856-0.970; P < 0.001) and >0.859 with an AUC 0.744 (95% CI: 0.587-0.901; P = 0.013) could predict causative parathyroid glands in the autografted forearm and the neck or mediastinum with diagnostic accuracies of 81.1% and 83.3%, respectively. Therefore, we propose that the intact PTH ratio is useful for predicting the localization of causative parathyroid glands for re-parathyroidectomy.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Tominaga Y, Katayama A, Sato T, Matsuoka S, Goto N, Haba T, et al.. Re-operation is frequently required when parathyroid glands remain after initial parathyroidectomy for advanced secondary hyperparathyroidism in uraemic patients. Nephrol Dial Transplant. 2003;18: 65–70. 10.1093/ndt/gfg1017 - DOI - PubMed
-
- de Andrade JS, Mangussi-Gomes JP, da Rocha LA, Ohe MN, Rosano M, das Neves MC, et al.. Localization of ectopic and supernumerary parathyroid glands in patients with secondary and tertiary hyperparathyroidism: surgical description and correlation with preoperative ultrasonography and Tc99m-Sestamibi scintigraphy. Braz J Otorhinolaryngol. 2014;80: 29–34. 10.5935/1808-8694.20140008 - DOI - PMC - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
