

Rapid diagnostic tests for the detection of recent dengue infections: An evaluation of six kits on clinical specimens
- PMID: 33793682
- PMCID: PMC8016316
- DOI: 10.1371/journal.pone.0249602
Rapid diagnostic tests for the detection of recent dengue infections: An evaluation of six kits on clinical specimens
Abstract
Introduction: Early and rapid confirmation of dengue infections strengthens disease surveillance program and are critical to the success of vector control measures. Rapid diagnostics tests (RDTs) are increasingly used to confirm recent dengue infections due to their ease of use and short turnaround time for results. Several studies undertaken in dengue-endemic Southeast Asia have reported the performance of RDTs against enzyme-linked immunosorbent assay (ELISA), reverse transcriptase polymerase chain reaction (RT-PCR) and virus isolation methods. However, few studies have compared multiple RDTs for the detection of dengue NS1 antigen and IgM antibody in a single combo cassette. We evaluated six RDTs in Singapore for their utility in routine clinical testing to detect recent dengue infections.
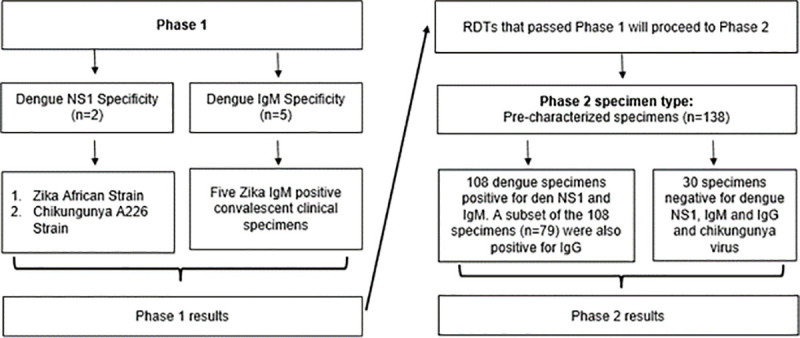
Methods: The evaluation comprised two phases. The first phase sought to determine each RDT's specificity to dengue NS1 and IgM using zika and chikungunya virus supernatant and zika convalescent samples. RDTs that cross-reacted with zika or chikungunya were not further tested in phase 2. The second phase sought to determine the sensitivity and specificity of the remaining RDTs to dengue NS1 and IgM using pre-characterised dengue specimens and non-dengue/chikungunya febrile clinical specimens.
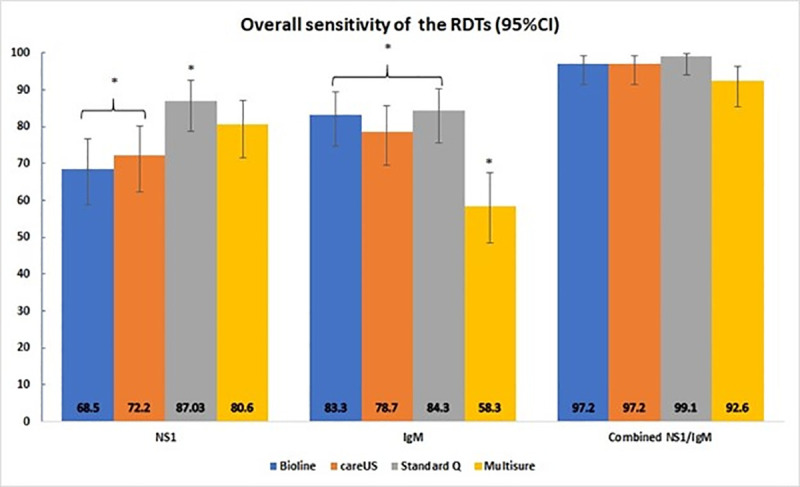
Results: None of the RDTs cross-reacted with zika IgM in Phase 1. Truquick and Quickprofile cross reacted with zika and chikungunya viruses and were not evaluated thereafter. Standard Q had the highest dengue NS1 and IgM sensitivity at 87.0% and 84.3% respectively whereas Bioline (68.5%) and Multisure (58.3%) had the lowest dengue NS1 and IgM sensitivity respectively. Combining dengue NS1/IgM detection results greatly improved the RDT ability to detect recent dengue infection; Standard Q had the highest sensitivity at 99.1% while Multisure had the lowest at 92.6%. All the RDTs were highly specific for dengue NS1 and IgM (96.7% to 100%). All the RDTs had high positive predictive values (98.4% to 100%) for NS1, IgM and combined NS1/IgM parameters whereas Standard Q had the highest negative predictive values at 68.2% (NS1), 63.8% (IgM) and 96.8% (NS1/IgM). For the RDTs, detection of NS1 declined from acute to convalescent phase of illness whereas IgM detection rate gradually increased over time.
Conclusion: In our study, several RDTs were evaluated for their diagnostic accuracy and capability in detecting recent dengue infection. Standard Q demonstrated a high degree of diagnostic accuracy and capability in the detection of NS1 and IgM biomarkers. RDTs can provide rapid and accurate confirmation of recent dengue infections and augment dengue surveillance and control programmes. Further studies are required to assess the usefulness of these RDTs in other epidemiology settings.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Gubler DJ. Emerging vector-borne flavivirus diseases: Are vaccines the solution? 2011;10(5):563–5. - PubMed
-
- Koh B, Ng LC, Kita Y, Tang C, Ang L, Wong K, et al. The 2005 dengue epidemic in Singapore: Epidemiology, prevention and control. Annals of the Academy of Medicine, Singapore. 2008;37:538–45. - PubMed
-
- World Health O. Dengue guidelines for diagnosis, treatment, prevention and control: new edition. Geneva: World Health Organization; 2009. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
