

Cost-effectiveness of immediate total-body CT in patients with severe trauma (REACT-2 trial)
- PMID: 33793734
- PMCID: PMC10364909
- DOI: 10.1093/bjs/znaa091
Cost-effectiveness of immediate total-body CT in patients with severe trauma (REACT-2 trial)
Abstract
Background: The effect of immediate total-body CT (iTBCT) on health economic aspects in patients with severe trauma is an underreported issue. This study determined the cost-effectiveness of iTBCT compared with conventional radiological imaging with selective CT (standard work-up (STWU)) during the initial trauma evaluation.
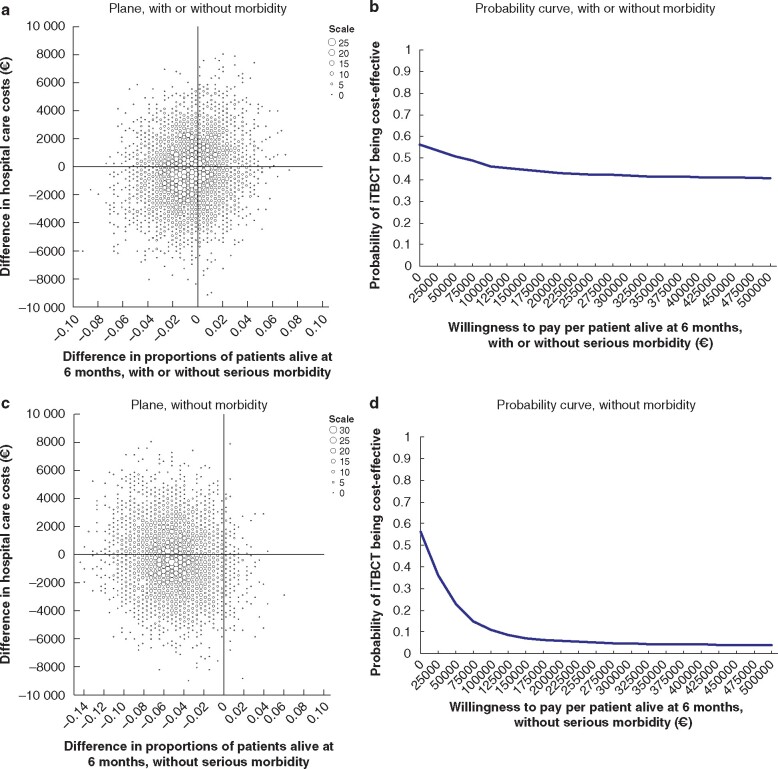
Methods: In this multicentre RCT, adult patients with a high suspicion of severe injury were randomized in-hospital to iTBCT or STWU. Hospital healthcare costs were determined for the first 6 months after the injury. The probability of iTBCT being cost-effective was calculated for various levels of willingness-to-pay per extra patient alive.
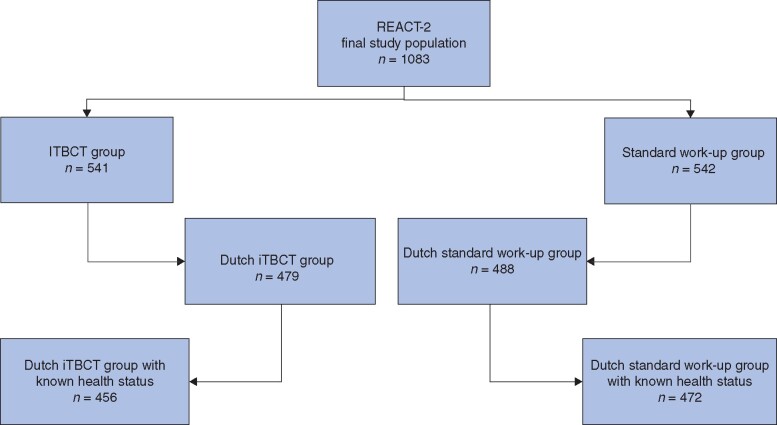
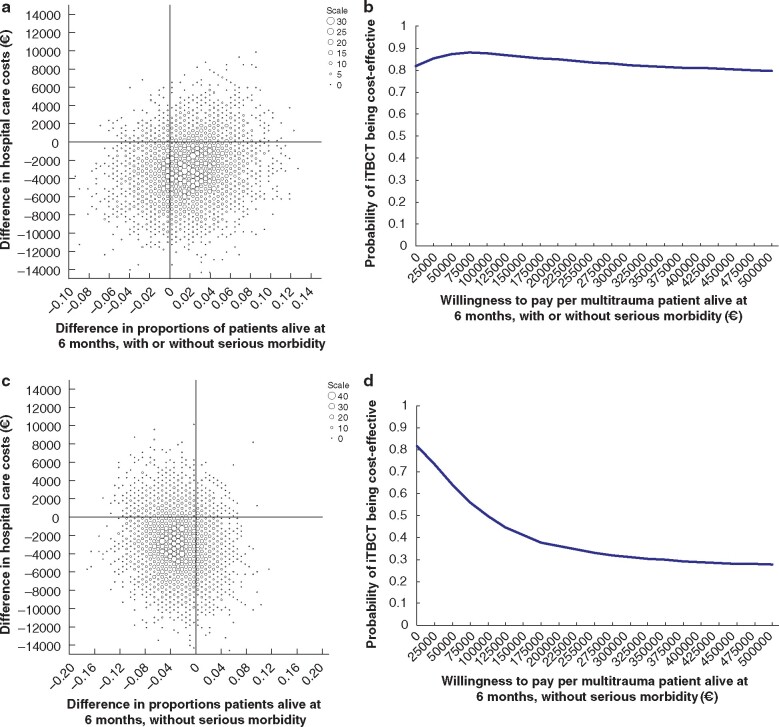
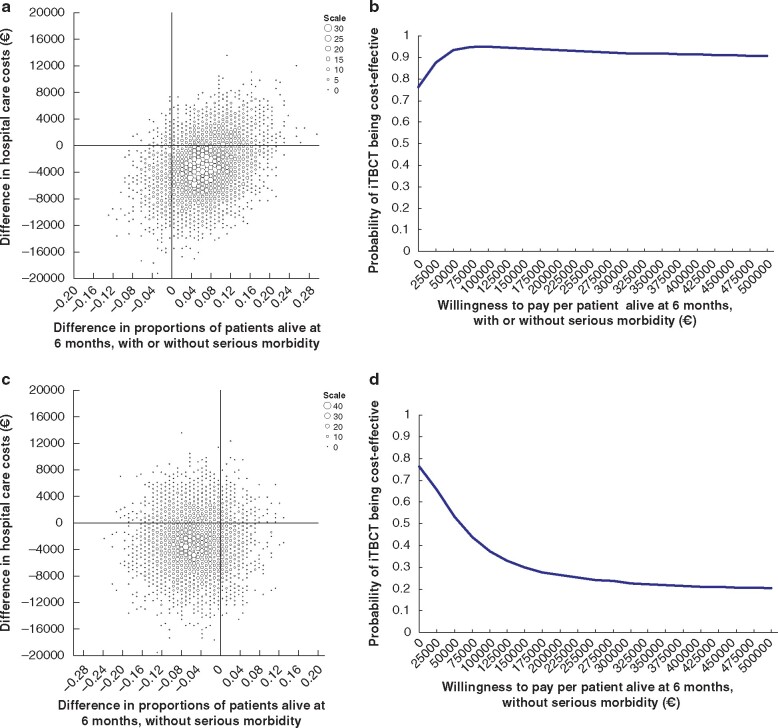
Results: A total of 928 Dutch patients with complete clinical follow-up were included. Mean costs of hospital care were €25 809 (95 per cent bias-corrected and accelerated (bca) c.i. €22 617 to €29 137) for the iTBCT group and €26 155 (€23 050 to €29 344) for the STWU group, a difference per patient in favour of iTBCT of €346 (€4987 to €4328) (P = 0.876). Proportions of patients alive at 6 months were not different. The proportion of patients alive without serious morbidity was 61.6 per cent in the iTBCT group versus 66.7 per cent in the STWU group (difference -5.1 per cent; P = 0.104). The probability of iTBCT being cost-effective in keeping patients alive remained below 0.56 for the whole group, but was higher in patients with multiple trauma (0.8-0.9) and in those with traumatic brain injury (more than 0.9).
Conclusion: Economically, from a hospital healthcare provider perspective, iTBCT should be the diagnostic strategy of first choice in patients with multiple trauma or traumatic brain injury.
Antecedentes: El efecto de la tomografía computarizada inmediata de todo el cuerpo (immediate total-body CT, iTBCT) sobre los aspectos económicos de la salud en pacientes con traumatismos graves es un tema con información limitada. Este estudio determinó el coste-efectividad de la exploración iTBCT en comparación con las imágenes radiológicas convencionales y la CT selectiva (evaluación estándar, standard work-up, STWU) durante la evaluación inicial del trauma.
Métodos: En este ensayo clínico aleatorizado y multicéntrico, los pacientes adultos con una alta sospecha de lesiones graves, una vez ingresados en el hospital, se asignaron al azar a una exploración iTBCT o STWU. Los costes de atención médica hospitalaria se determinaron durante los primeros seis meses posteriores al trauma. La probabilidad de que iTBCT fuera coste-efectiva se calculó para varios niveles de disposición a pagar por cada paciente adicional vivo.
Resultados: Se incluyeron un total de 928 pacientes holandeses con seguimiento clínico completo. Los costes medios de la atención hospitalaria fueron 25.809€ (95% bcaCI: 22.617€ a 29.137€) para el grupo iTBCT y 26.155€ (95% bcaCI: 23.050€ a 29.344€) para el grupo STWU, una diferencia de 346€ por paciente en favor de iTBCT (95% bcaCI: 4.987€ a 4.328€; P = 0,876). El porcentaje de pacientes vivos a los seis meses no fue diferente. La diferencia en el porcentaje de pacientes vivos sin morbilidad grave fue del 61,6% en el grupo iTBCT versus 66,7% en el grupo STWU (-5,1%, P = 0,104). La probabilidad de que iTBCT fuese costo-eficiente para mantener a los pacientes en vida se mantuvo por debajo de 0,56 en todo el grupo, sin embargo, fue mayor en pacientes politraumatizados (0,8-0,9) y en pacientes con lesión cerebral traumática (más de 0,9).
Conclusión: Desde la perspectiva económica del proveedor de atención médica hospitalaria, la tomografía computarizada inmediata de todo el cuerpo debería ser la estrategia diagnóstica de primera elección en pacientes con traumatismos múltiples o traumatismos craneoencefálicos.
© The Author(s) 2021. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures
References
-
- Sierink JC, Treskes K, Edwards MJ, Beuker BJ, den Hartog D, Hohmann J et al. Immediate total-body CT scanning versus conventional imaging and selective CT scanning in patients with severe trauma (REACT-2): a randomised controlled trial. Lancet 2016;388:673–683 - PubMed
-
- American College of Surgeons Committee on Trauma. ATLS, Advanced Trauma Life Support Program for Doctors. Chicago: ACS, 2018.
-
- Hakkaart-Van Roijen L, Tan SS, Bouwmans CAM (eds). [Guideline for Costing Research. Methods and Standard Unit Costs for Economic Evaluation in Health Care (actualized version edition).] Rotterdam: Erasmus University, 2010.
-
- CBS StatLine. [Consumer Prices; September 2014.] http://Statline.cbs.nl/StatWeb/publications/?PA=71311ned (accessed 11 February 2016).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
