

A link between gastrointestinal disorders and migraine: Insights into the gut-brain connection
- PMID: 33793965
- PMCID: PMC8251535
- DOI: 10.1111/head.14099
A link between gastrointestinal disorders and migraine: Insights into the gut-brain connection
Abstract
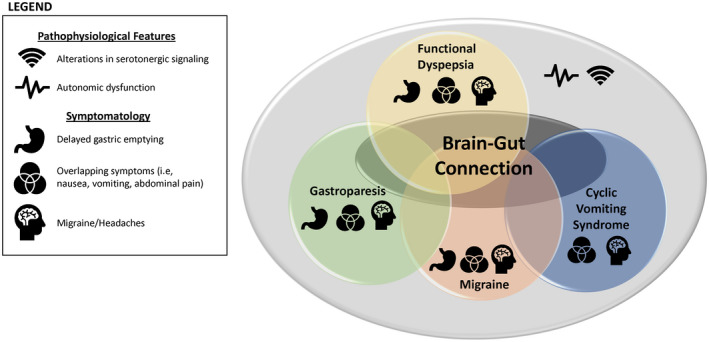
Background: Migraine is a complex, multifaceted, and disabling headache disease that is often complicated by gastrointestinal (GI) conditions, such as gastroparesis, functional dyspepsia, and cyclic vomiting syndrome (CVS). Functional dyspepsia and CVS are part of a spectrum of disorders newly classified as disorders of gut-brain interaction (DGBI). Gastroparesis and functional dyspepsia are both associated with delayed gastric emptying, while nausea and vomiting are prominent in CVS, which are also symptoms that commonly occur with migraine attacks. Furthermore, these gastric disorders are comorbidities frequently reported by patients with migraine. While very few studies assessing GI disorders in patients with migraine have been performed, they do demonstrate a physiological link between these conditions.
Objective: To summarize the available studies supporting a link between GI comorbidities and migraine, including historical and current scientific evidence, as well as provide evidence that symptoms of GI disorders are also observed outside of migraine attacks during the interictal period. Additionally, the importance of route of administration and formulation of migraine therapies for patients with GI symptoms will be discussed.
Methods: A literature search of PubMed for articles relating to the relationship between the gut and the brain with no restriction on the publication year was performed. Studies providing scientific support for associations of gastroparesis, functional dyspepsia, and CVS with migraine and the impact these associations may have on migraine treatment were the primary focus. This is a narrative review of identified studies.
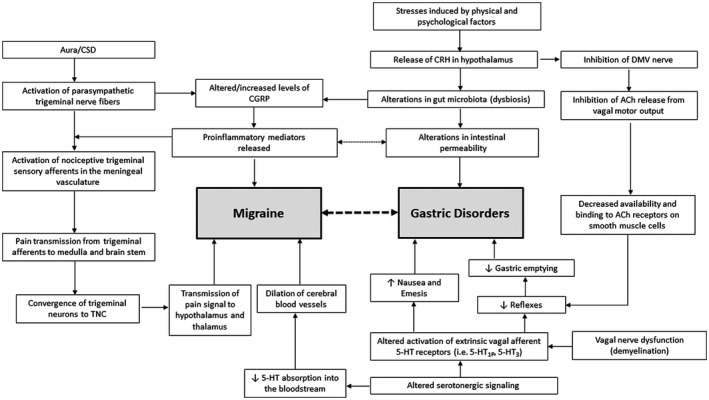
Results: Although the association between migraine and GI disorders has received very little attention in the literature, the existing evidence suggests that they may share a common etiology. In particular, the relationship between migraine, gastric motility, and vomiting has important clinical implications in the treatment of migraine, as delayed gastric emptying and vomiting may affect oral dosing compliance, and thus, the absorption and efficacy of oral migraine treatments.
Conclusions: There is evidence of a link between migraine and GI comorbidities, including those under the DGBI classification. Many patients do not find adequate relief with oral migraine therapies, which further necessitates increased recognition of GI disorders in patients with migraine by the headache community.
Keywords: cyclic vomiting syndrome; disorders of gut-brain interaction; functional dyspepsia; gastric motility; gastroparesis; migraine.
© 2021 The Authors. Headache: The Journal of Head and Face Pain published by Wiley Periodicals LLC on behalf of American Headache Society.
Conflict of interest statement
Sheena K. Aurora, Sutapa Ray, and Stephen B. Shrewsbury are full‐time employees of Impel NeuroPharma and are stockholders in Impel NeuroPharma. Nada Hindiyeh serves on advisory boards for Amgen, Eli Lilly, Lundbeck, and Zosano Pharma. Linda Nguyen serves on an advisory board for Gemelli and consults for Pendulum, Neurogastrx, Ironwood, Eli Lilly, and Alnylam.
Figures
References
-
- Headache Classification Committee of the International Headache Society (IHS) . The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38:1‐211. - PubMed
-
- Lipton RB, Buse DC, Saiers J, Fanning KM, Serrano D, Reed ML. Frequency and burden of headache‐related nausea: results from the American Migraine Prevalence and Prevention (AMPP) study. Headache. 2013;53:93‐103. - PubMed
-
- Aamodt AH, Stovner LJ, Hagen K, Zwart JA. Comorbidity of headache and gastrointestinal complaints. The Head‐HUNT Study. Cephalalgia. 2008;28:144‐151. - PubMed
-
- Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646‐657. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
