

Duration of cytopenias with concomitant venetoclax and azole antifungals in acute myeloid leukemia
- PMID: 33793970
- PMCID: PMC8249340
- DOI: 10.1002/cncr.33508
Duration of cytopenias with concomitant venetoclax and azole antifungals in acute myeloid leukemia
Abstract
Background: Venetoclax (VEN) combined with the hypomethylating agent (HMA) azacitidine improves survival in patients aged ≥75 years with newly diagnosed acute myeloid leukemia (AML). VEN and HMA treatment can result in prolonged and often profound neutropenia, and this warrants antifungal prophylaxis. Azole antifungals inhibit cytochrome P450 3A4, the primary enzyme responsible for VEN metabolism; this results in VEN dose reductions for each concomitant antifungal. Limited clinical data exist on outcomes for patients treated with VEN, an HMA, and various azoles.
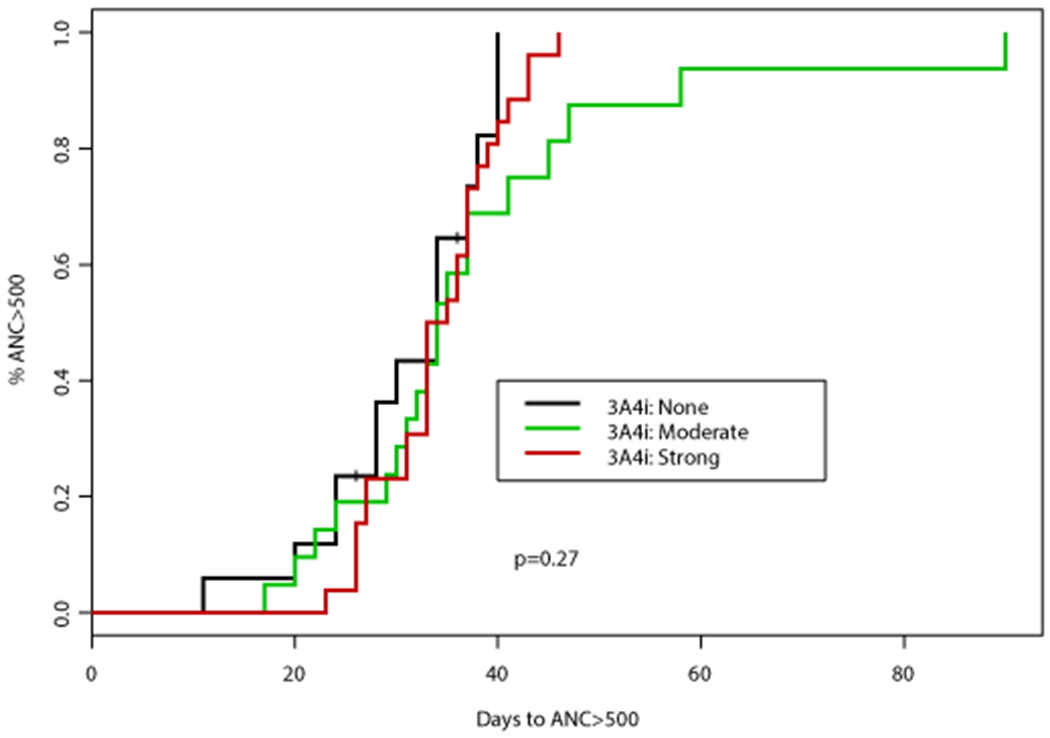
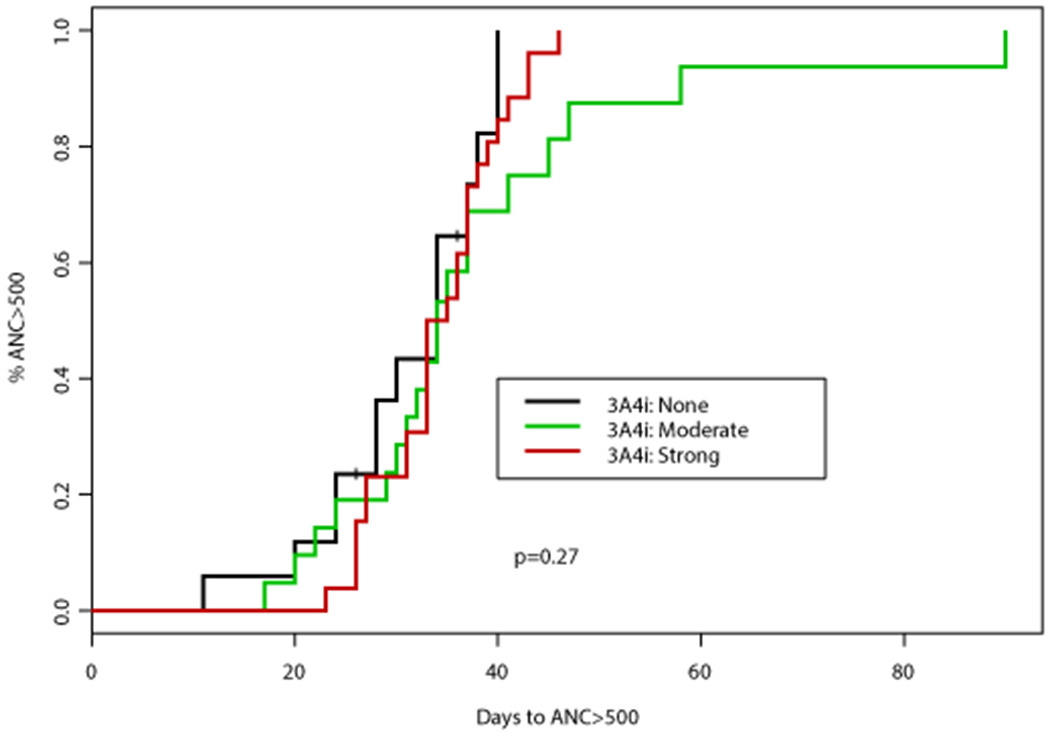
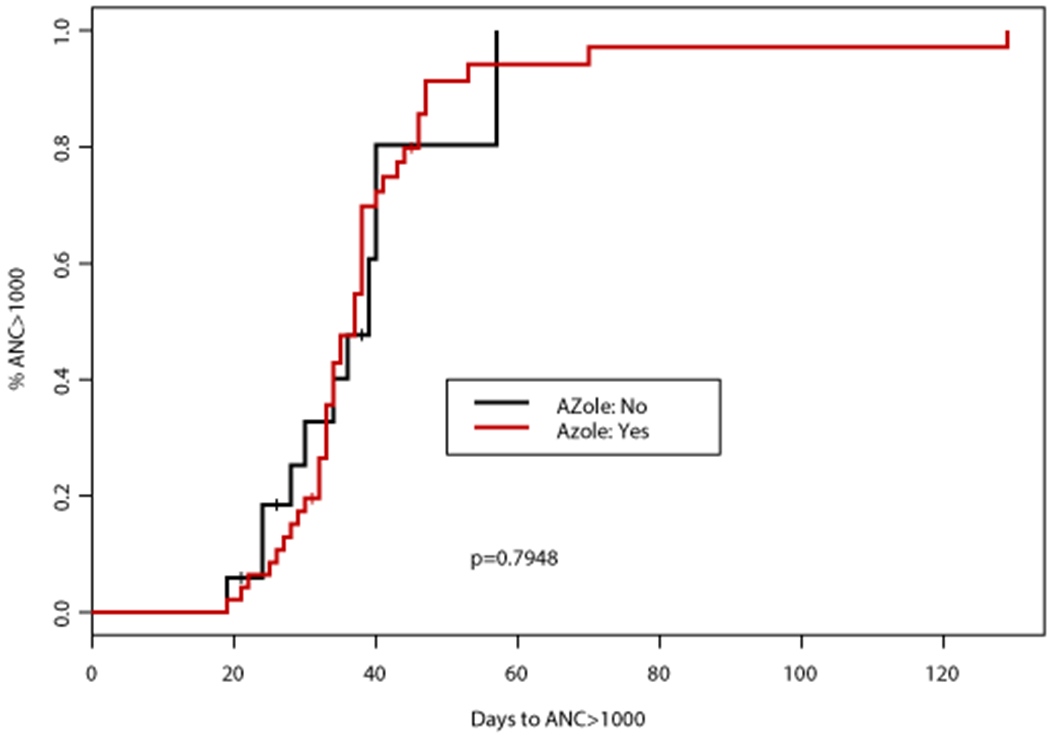
Methods: The time to neutrophil recovery (absolute neutrophil count [ANC] > 1000 cells/mm3 ) and platelet (PLT) recovery (PLT count > 100,000 cells/mm3 ) in 64 patients with newly diagnosed AML who achieved a response after course 1 of VEN plus an HMA were evaluated. HMA therapy included azacitidine (75 mg/m2 intravenously/subcutaneously for 7 days) or decitabine (20 mg/m2 intravenously for 5 or 10 days).
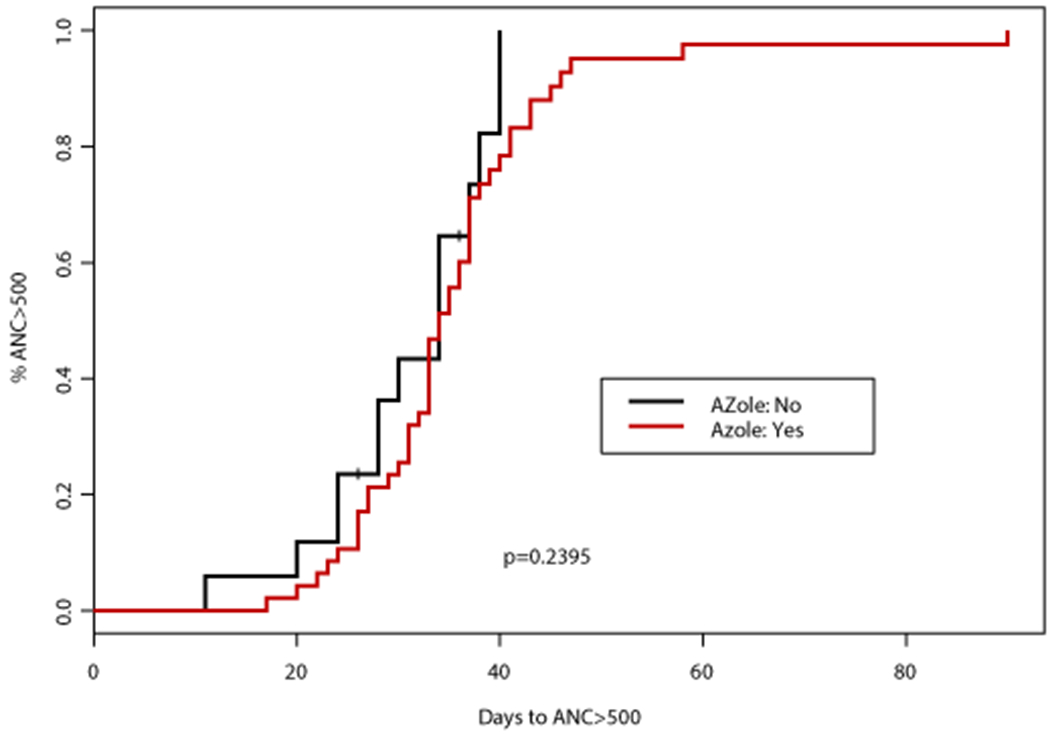
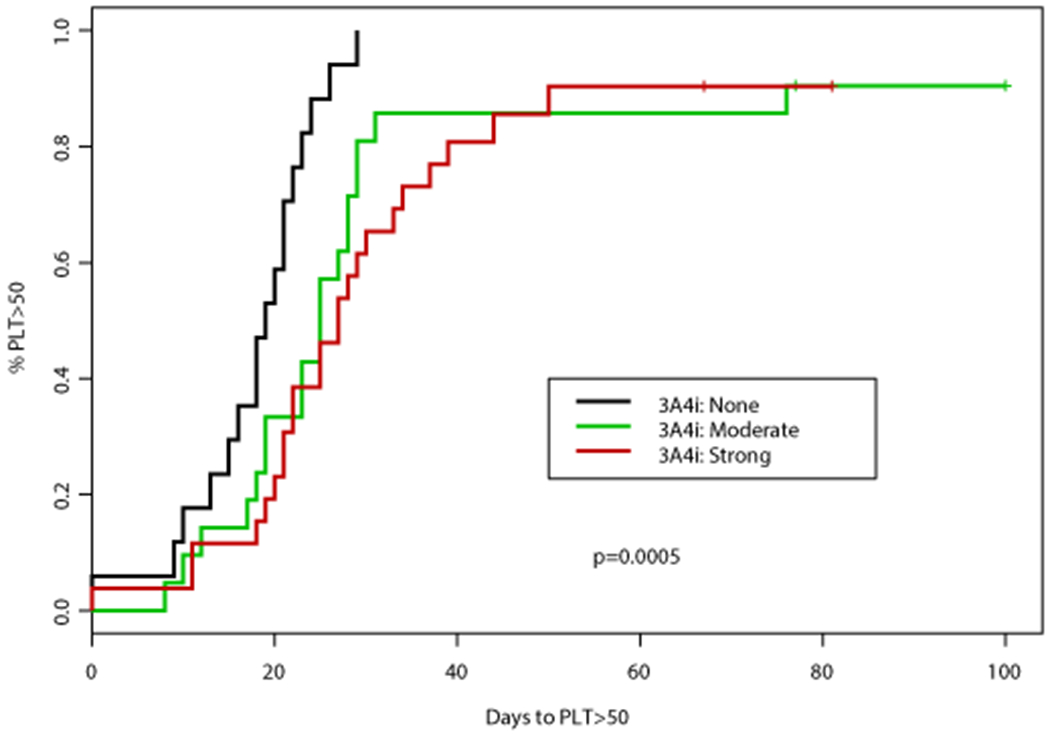
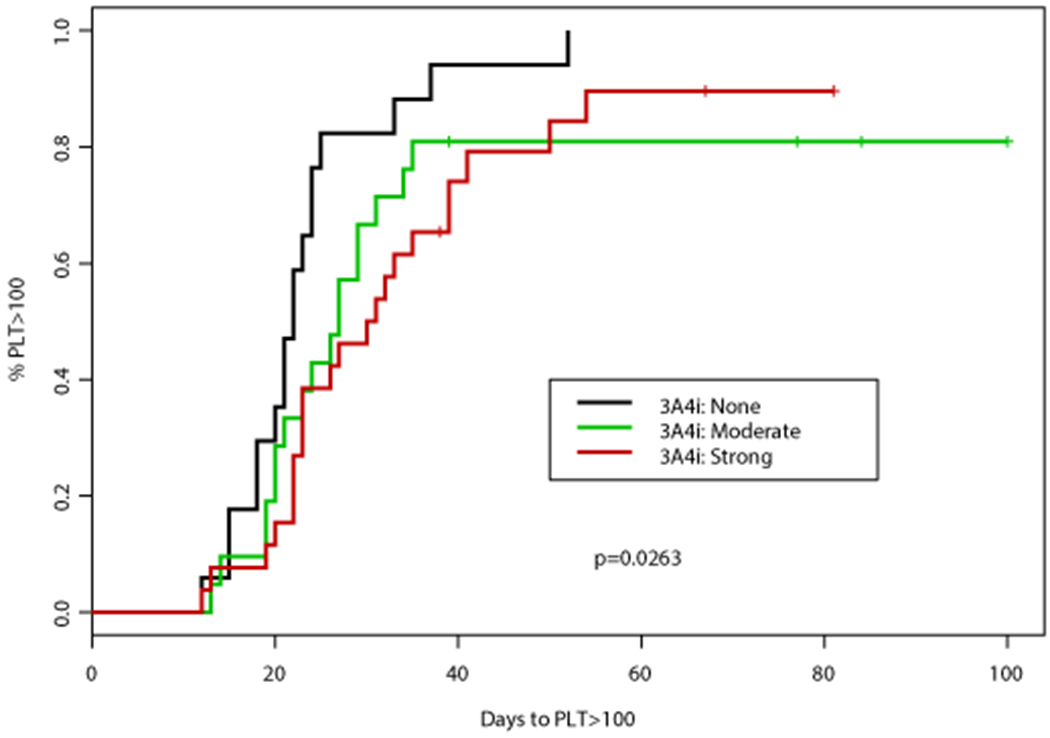
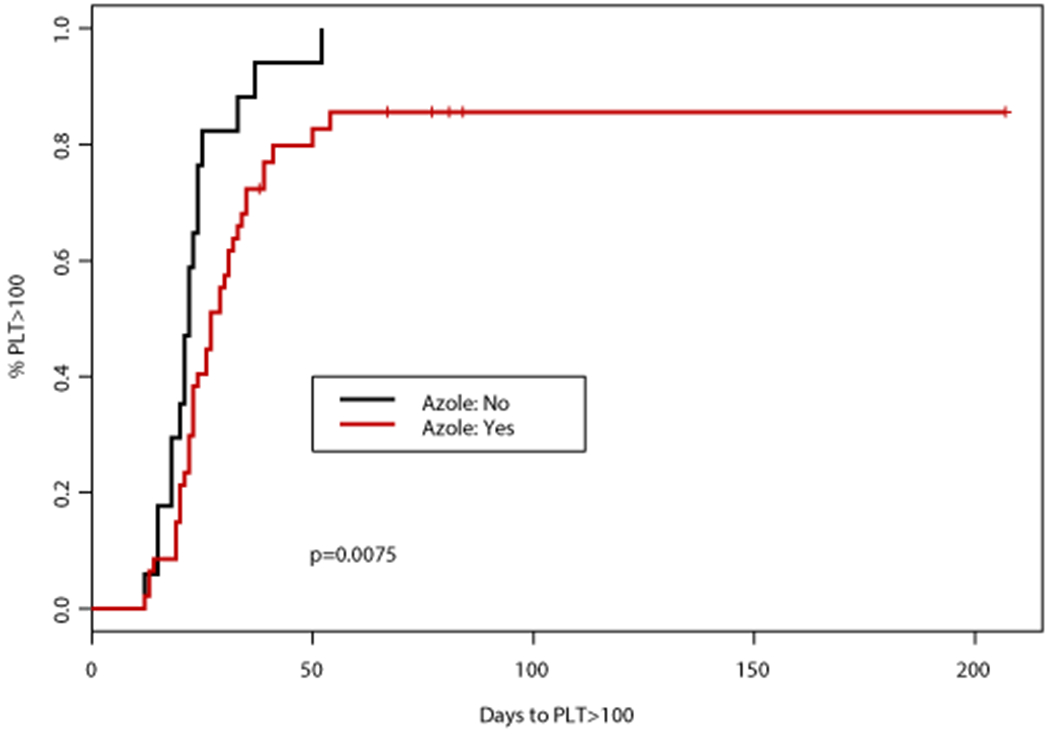
Results: Forty-seven patients (73%) received an azole: posaconazole (n = 17; 27%), voriconazole (n = 9; 14%), isavuconazole (n = 20; 31%), or fluconazole (n = 1; 2%). The median time to ANC recovery were similar for patients who did receive an azole (37 days; 95% confidence interval [CI], 34-38 days) and patients who did not receive an azole (39 days; 95% CI, 30 days to not estimable; P = .8). The median time to PLT recovery was significantly longer for patients receiving azoles (28 vs 22 days; P = .01). The median times to ANC recovery (35 vs 38 days) and PLT recovery (26 vs 32 days) were similar with posaconazole and voriconazole.
Conclusions: VEN plus an HMA resulted in neutropenia and thrombocytopenia, with the latter prolonged in patients receiving concomitant azoles. Concomitant posaconazole or voriconazole and VEN (100 mg) resulted in similar ANC and PLT recovery times, suggesting the safety of these dosage combinations during course 1.
Keywords: acute myeloid leukemia; azole antifungals; invasive fungal infection; prophylaxis; venetoclax.
© 2021 American Cancer Society.
Figures
References
-
- N H, AM N, M K, et al. SEER Cancer Statistics Review, 1975-2013. Accessed December, 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
