

Protocolized Postextubation Respiratory Support to Prevent Reintubation: A Randomized Clinical Trial
- PMID: 33794131
- PMCID: PMC8513595
- DOI: 10.1164/rccm.202009-3561OC
Protocolized Postextubation Respiratory Support to Prevent Reintubation: A Randomized Clinical Trial
Abstract
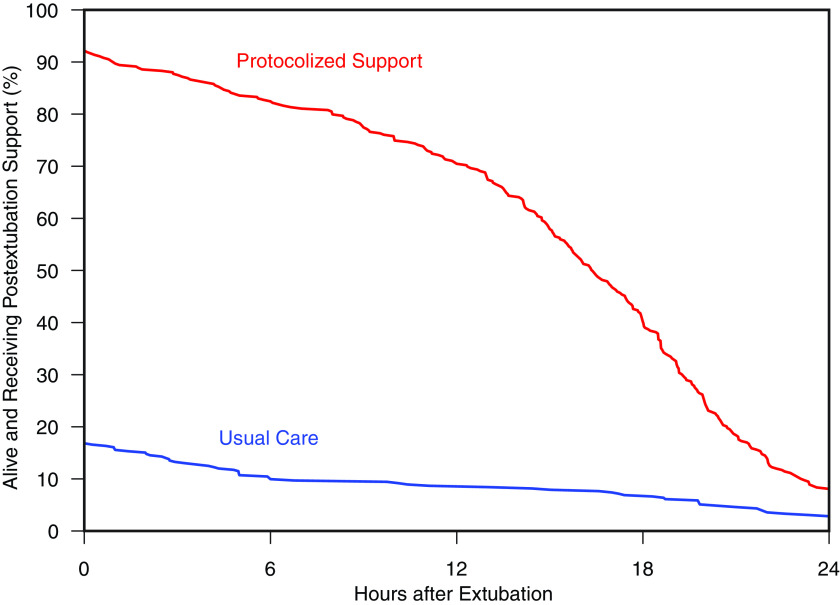
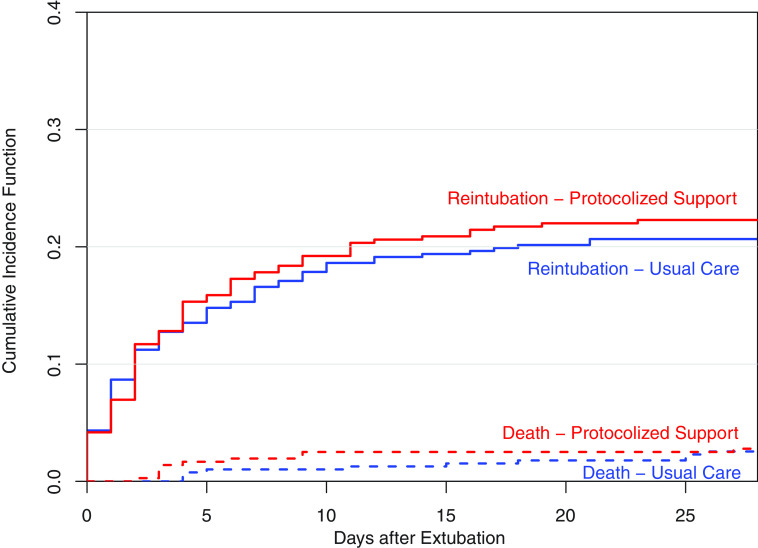
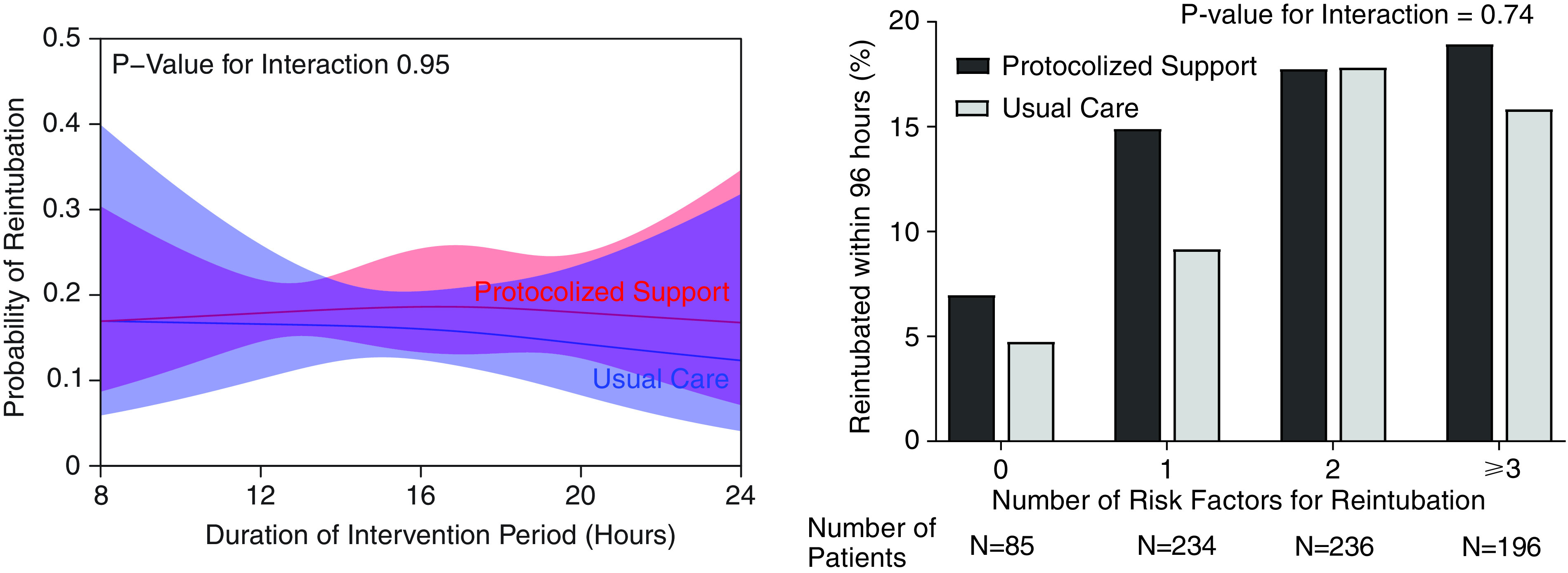
Rationale: Respiratory support (noninvasive ventilation or high-flow nasal cannula) applied at the time of extubation has been reported to reduce reintubation rates, but concerns regarding effectiveness have limited uptake into practice.Objectives: To determine if providing postextubation respiratory support to all patients undergoing extubation in a medical ICU would decrease the incidence of reintubation.Methods: We conducted a pragmatic, two-armed, cluster-crossover trial of adults undergoing extubation from invasive mechanical ventilation between October 1, 2017, and March 31, 2019, in the medical ICU of an academic medical center. Patients were assigned to either protocolized postextubation respiratory support (a respiratory therapist-driven protocol in which patients with suspected hypercapnia received noninvasive ventilation and patients without suspected hypercapnia received high-flow nasal cannula) or usual care (postextubation management at the discretion of treating clinicians). The primary outcome was reintubation within 96 hours of extubation.Measurements and Main Results: A total of 751 patients were enrolled. Of the 359 patients assigned to protocolized support, 331 (92.2%) received postextubation respiratory support compared with 66 of 392 patients (16.8%) assigned to usual care, a difference driven by differential use of high-flow nasal cannula (74.7% vs. 2.8%). A total of 57 patients (15.9%) in the protocolized support group experienced reintubation compared with 52 patients (13.3%) in the usual care group (odds ratio, 1.23; 95% confidence interval, 0.82 to 1.84; P = 0.32).Conclusions: Among a broad population of critically ill adults undergoing extubation from invasive mechanical ventilation at an academic medical center, protocolized postextubation respiratory support, primarily characterized by an increase in the use of high-flow nasal cannula, did not prevent reintubation compared with usual care.Clinical trial registered with www.clinicaltrials.gov (NCT0328831).
Trial registration: ClinicalTrials.gov NCT03288311.
Keywords: invasive mechanical ventilation; noninvasive respiratory support; reintubation.
Figures
Comment in
-
Postextubation Respiratory Support: Of Clinical Trials and Clinical Decisions.Am J Respir Crit Care Med. 2021 Aug 1;204(3):245-247. doi: 10.1164/rccm.202104-0844ED. Am J Respir Crit Care Med. 2021. PMID: 33901412 Free PMC article. No abstract available.
References
-
- Acute Respiratory Distress Syndrome Network. Brower RG. Matthay MA. Morris A. Schoenfeld D. Thompson BT. Wheeler A.. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. - PubMed
-
- Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000;342:1471–1477. - PubMed
-
- Ely EW, Baker AM, Dunagan DP, Burke HL, Smith AC, Kelly PT, et al. Effect on the duration of mechanical ventilation of identifying patients capable of breathing spontaneously. N Engl J Med. 1996;335:1864–1869. - PubMed
-
- Girard TD, Kress JP, Fuchs BD, Thomason JWW, Schweickert WD, Pun BT, et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): a randomised controlled trial. Lancet. 2008;371:126–134. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
