

Antihypertensive treatment and risk of cancer: an individual participant data meta-analysis
- PMID: 33794209
- PMCID: PMC8024901
- DOI: 10.1016/S1470-2045(21)00033-4
Antihypertensive treatment and risk of cancer: an individual participant data meta-analysis
Abstract
Background: Some studies have suggested a link between antihypertensive medication and cancer, but the evidence is so far inconclusive. Thus, we aimed to investigate this association in a large individual patient data meta-analysis of randomised clinical trials.
Methods: We searched PubMed, MEDLINE, The Cochrane Central Register of Controlled Trials, and ClinicalTrials.gov from Jan 1, 1966, to Sept 1, 2019, to identify potentially eligible randomised controlled trials. Eligible studies were randomised controlled trials comparing one blood pressure lowering drug class with a placebo, inactive control, or other blood pressure lowering drug. We also required that trials had at least 1000 participant years of follow-up in each treatment group. Trials without cancer event information were excluded. We requested individual participant data from the authors of eligible trials. We pooled individual participant-level data from eligible trials and assessed the effects of angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor blockers (ARBs), β blockers, calcium channel blockers, and thiazide diuretics on cancer risk in one-stage individual participant data and network meta-analyses. Cause-specific fixed-effects Cox regression models, stratified by trial, were used to calculate hazard ratios (HRs). The primary outcome was any cancer event, defined as the first occurrence of any cancer diagnosed after randomisation. This study is registered with PROSPERO (CRD42018099283).
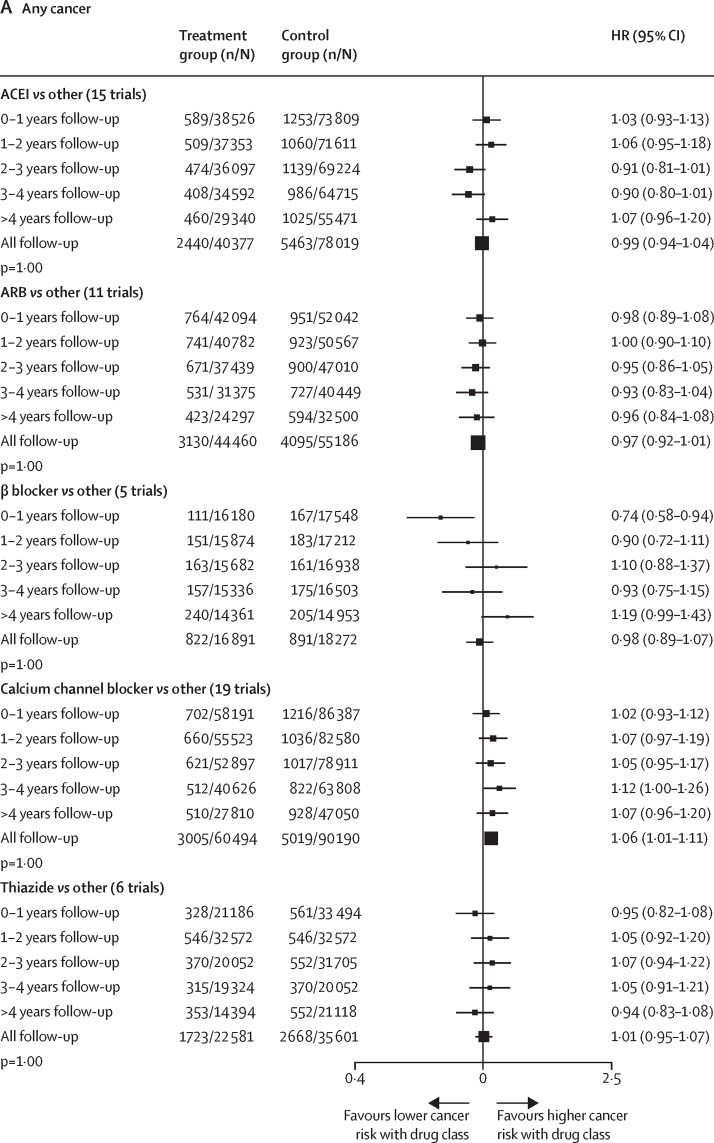
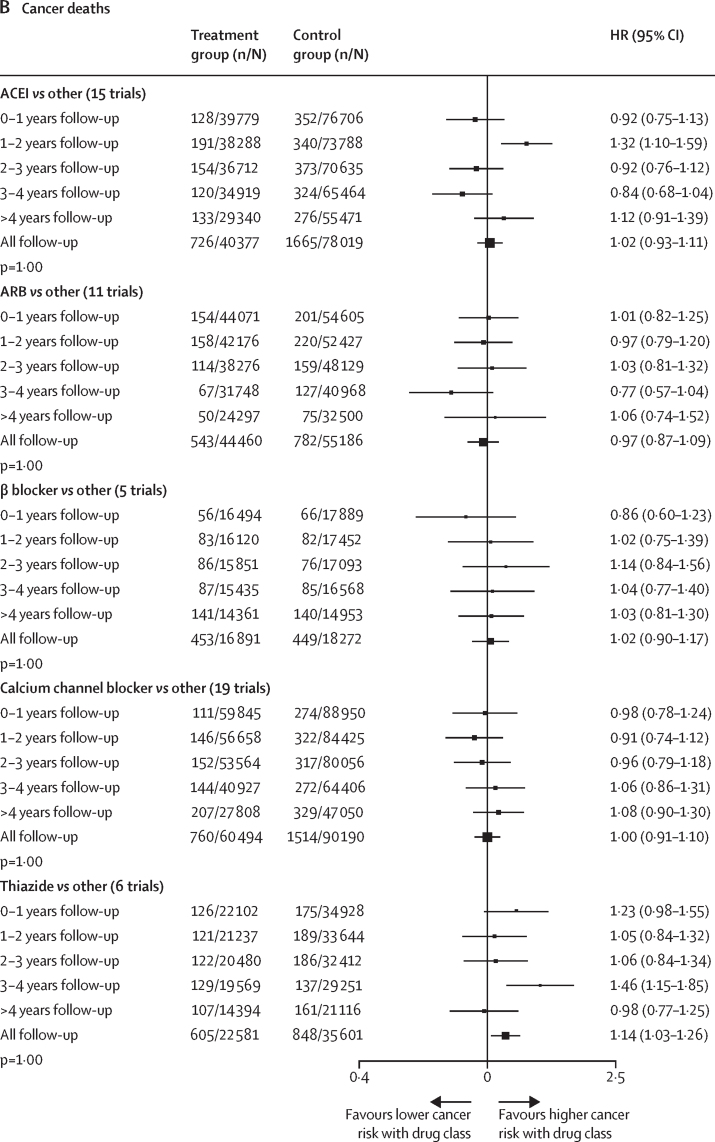
Findings: 33 trials met the inclusion criteria, and included 260 447 participants with 15 012 cancer events. Median follow-up of included participants was 4·2 years (IQR 3·0-5·0). In the individual participant data meta-analysis comparing each drug class with all other comparators, no associations were identified between any antihypertensive drug class and risk of any cancer (HR 0·99 [95% CI 0·95-1·04] for ACEIs; 0·96 [0·92-1·01] for ARBs; 0·98 [0·89-1·07] for β blockers; 1·01 [0·95-1·07] for thiazides), with the exception of calcium channel blockers (1·06 [1·01-1·11]). In the network meta-analysis comparing drug classes against placebo, we found no excess cancer risk with any drug class (HR 1·00 [95% CI 0·93-1·09] for ACEIs; 0·99 [0·92-1·06] for ARBs; 0·99 [0·89-1·11] for β blockers; 1·04 [0·96-1·13] for calcium channel blockers; 1·00 [0·90-1·10] for thiazides).
Interpretation: We found no consistent evidence that antihypertensive medication use had any effect on cancer risk. Although such findings are reassuring, evidence for some comparisons was insufficient to entirely rule out excess risk, in particular for calcium channel blockers.
Funding: British Heart Foundation, National Institute for Health Research, Oxford Martin School.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4·0 license. Published by Elsevier Ltd.. All rights reserved.
Figures


Comment in
-
Elucidating the association between antihypertensive drugs and cancer: a need for real-world studies.Lancet Oncol. 2021 Apr;22(4):421-422. doi: 10.1016/S1470-2045(21)00085-1. Lancet Oncol. 2021. PMID: 33794202 No abstract available.
References
-
- Turnbull F, Neal B, Algert C. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trials. Lancet. 2003;362:1527–1535. - PubMed
-
- Gascón JJ, Sánchez-Ortuño M, Llor B, Skidmore D, Saturno PJ. Why hypertensive patients do not comply with the treatment: results from a qualitative study. Fam Pract. 2004;21:125–130. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
