

Prevalence of Micronutrient Deficiency after Bariatric Surgery
- PMID: 33794530
- PMCID: PMC8138235
- DOI: 10.1159/000514847
Prevalence of Micronutrient Deficiency after Bariatric Surgery
Abstract
Introduction: While vitamin deficiency after bariatric surgery has been repeatedly described, few studies have focused on adequate micronutrient status. In this study, we examine the prevalence of vitamin and micronutrient deficiency for the first 3 years after surgery.
Methods: Out of 1,216 patients undergoing surgery, 485 who underwent postoperative follow-up in an outpatient clinic between 2010 and 2019 were included in this evaluation (76.9% women, mean age 42 ± 12 years, mean BMI: year 1, 33.9 ± 19.2; year 2, 29.7 ± 8.7; year 3, 26.2 ± 4.0). Weight and cardiovascular risk factors as well as ferritin, vitamin B12, folic acid, 25-OH-vitamin D, vitamin A, vitamin E, zinc, copper, and selenium were evaluated. Deficits were defined as follows: ferritin <15 µg/L, vitamin B12 <197 pg/mL, folic acid <4.4 ng/mL, 25-OH-vitamin D <75 nmol/L, vitamin A <1.05 µmol/L, vitamin E <12 µmol/L, zinc <0.54 mg/L, copper <0.81 mg/L, and selenium <50 µg/L. All patients underwent dietary counselling and substitution of the respective deficits as appropriate.
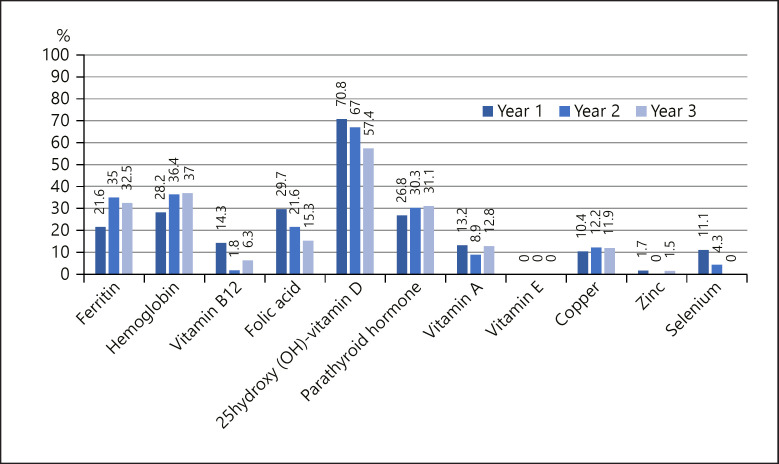
Results: One year after bariatric surgery, 485 patients completed follow-up. This number decreased to 114 patients in year 2, and 80 patients in year 3. Overall, 42.7% (n = 207) underwent sleeve gastrectomy, 43.7% (n = 211) Roux-en-Y-gastric bypass, and 13.9% (n = 67) gastric banding. The following deficits were found (year 1/2/3): ferritin, 21.6/35.0/32.5%; vitamin B12, 14.3/1.8/6.3%; folic acid, 29.7/21.6/15.3%; 25-OH-vitamin D, 70.8/67.0/57.4%; vitamin A, 13.2/8.9/12.8%; vitamin E, 0%; zinc, 1.7/0/1.5%; copper, 10.4/12.2/11.9%; selenium, 11.1/4.3/0%.
Conclusion: As seen in other studies, the follow-up frequency decreased over the years. Despite intensive substitution, the extent of some deficiencies increased or did not improve. These results suggest reinforcing measures to motivate patients for regular follow-up visits, considering closer monitoring schedules, and improving supplementation strategies.
Keywords: Bariatric surgery; Micronutrients; Roux-en-Y-gastric bypass; Sleeve gastrectomy; Vitamins.
© 2021 The Author(s) Published by S. Karger AG, Basel.
Conflict of interest statement
No potential conflicts of interest relevant to this article were reported. During the last 3 years E.-C.K. received honoraria for national lectures by the Austrian Obesity Society. J.M.B. received honoraria from AstraZeneca, Boehringer Ingelheim, Eli Lilly, MSD, Novo Nordisk, and Sanofi aventis. B.L. received grant support and honoraria for research projects and advice from Eli Lilly, Novo Nordisk, Sanofi, Boehringer Ingelheim, AstraZeneca, Bayer, Amgen. A.S. and V.P. have nothing to disclose.
Figures
References
-
- World Health Organisation Key Facts Available form: www.who.int/mediacentre/factsheets/fs311/en/
-
- Stein J, Stier C, Raab H, Weiner R. Review article: the nutritional and pharmacological consequences of obesity surgery. Aliment Pharmacol Ther. 2014 Sep;40((6)):582–609. - PubMed
-
- Ben-Porat T, Elazary R, Goldenshluger A, Sherf Dagan S, Mintz Y, Weiss R. Nutritional deficiencies four years after laparoscopic sleeve gastrectomy-are supplements required for a lifetime? Surg Obes Relat Dis. 2017 Jul;13((7)):1138–44. - PubMed
-
- Caron M, Hould FS, Lescelleur O, Marceau S, Lebel S, Julien F, et al. Long-term nutritional impact of sleeve gastrectomy. Surg Obes Relat Dis. 2017 Oct;13((10)):1664–73. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
