

Prevalence of children born small for gestational age with short stature who qualify for growth hormone treatment
- PMID: 33794966
- PMCID: PMC8015030
- DOI: 10.1186/s13052-021-01026-3
Prevalence of children born small for gestational age with short stature who qualify for growth hormone treatment
Abstract
Background: Recombinant human growth hormone (rhGH) is approved in Europe as a treatment for short children born small for gestational age (SGA) since 2003. However, no study evaluated the prevalence of SGA children with short stature who qualify for rhGH in Europe so far. This study aimed to investigate in an Italian population the prevalence of children born SGA, of short stature in children born SGA, and of SGA children who qualify for rhGH treatment at 4 years of age.
Methods: We conducted a population-based study on primary care pediatricians' databases in Trieste, Italy. Data was collected on 3769 children born between 2004 and 2014. SGA was defined as birth weight and/or birth length ≤ - 2 SDS. Data on height and weight were registered at the closest well-being visit to 1, 2, 3, 4 years of age. Short stature was defined as height ≤ - 2 SDS. Short children born SGA who qualify for rhGH treatment were identified according to Note AIFA #39 criteria (age ≥ 4 years; height ≤ - 2.5 SDS; growth velocity < 50th percentile).
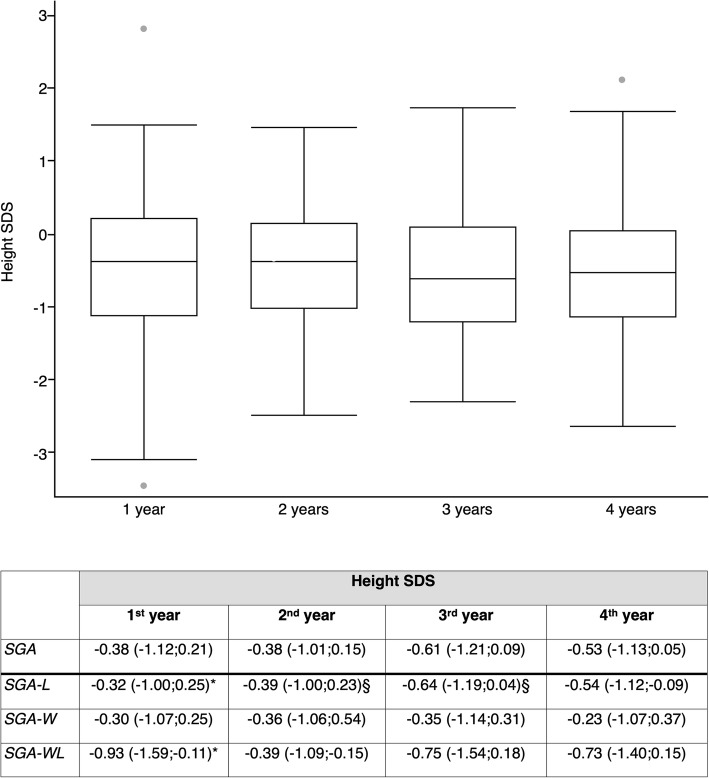
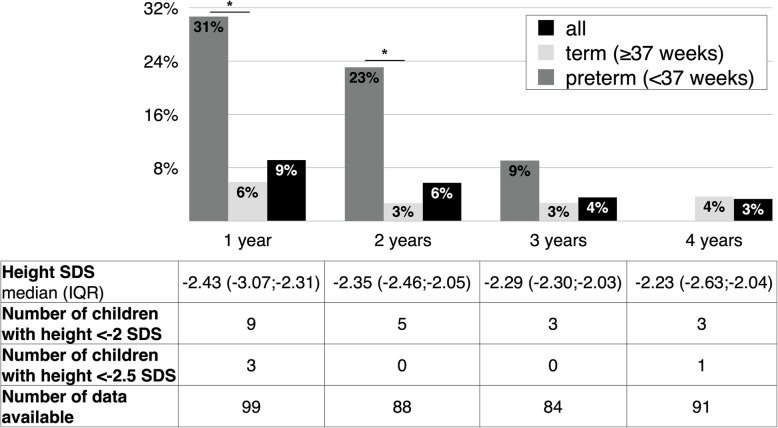
Results: Full data at birth were available for 3250 children. The SGA prevalence was 3.6% (0.8% SGA for weight, 2.2% SGA for length, 0.6% SGA for both weight and length). The prevalence of short stature among SGA children was 9% at 1 year of age, 6% at 2 years (significantly higher in preterm in the first 2 years), 4% at 3 years, 3% at 4 years (all born at term). At 4 years of age, median height SDS was - 0.52. One child born SGA was eligible for GH treatment (0.8% among SGA children).
Conclusions: The prevalence in a general pediatric population of children born SGA who qualify for GH treatment was 1:3250. Although the prevalence of SGA in our population was similar to previous studies, catch-up growth was recorded earlier in our sample compared to previous reports, and term babies had late catch-up. Height SDS of children born SGA at 4 years of age was lower than expected (- 0.52 SDS).
Keywords: Catch-up growth; Growth hormone; Italy; Short stature; Small-for-gestational age.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Prevalence of small for gestational age (SGA) and short stature in children born SGA who qualify for growth hormone treatment at 3 years of age: Population-based study.Pediatr Int. 2016 May;58(5):372-6. doi: 10.1111/ped.12859. Epub 2016 Feb 19. Pediatr Int. 2016. PMID: 26617415
-
Adult height of children born small for gestational age treated with growth hormone and gonadotropin-releasing hormone analogs in Southern Brazil.Arch Endocrinol Metab. 2025 Feb 24;69(1):e230513. doi: 10.20945/2359-4292-2023-0513. Arch Endocrinol Metab. 2025. PMID: 39992732 Free PMC article.
-
Children born small-for-gestational age: postnatal growth and hormonal status.Horm Res. 1998;49 Suppl 2:7-13. doi: 10.1159/000053080. Horm Res. 1998. PMID: 9730665
-
International Small for Gestational Age Advisory Board consensus development conference statement: management of short children born small for gestational age, April 24-October 1, 2001.Pediatrics. 2003 Jun;111(6 Pt 1):1253-61. doi: 10.1542/peds.111.6.1253. Pediatrics. 2003. PMID: 12777538 Review.
-
Latin American consensus: children born small for gestational age.BMC Pediatr. 2011 Jul 19;11:66. doi: 10.1186/1471-2431-11-66. BMC Pediatr. 2011. PMID: 21771322 Free PMC article.
Cited by
-
Growth hormone effect on body composition of children born small for gestational age: a systematic review.J Pediatr (Rio J). 2023 May-Jun;99(3):219-227. doi: 10.1016/j.jped.2022.11.010. Epub 2022 Dec 27. J Pediatr (Rio J). 2023. PMID: 36584978 Free PMC article.
-
Gestational Diabetes Mellitus and Small-for-Gestational-Age: An Insight into the Placental Molecular Biomarkers.Int J Mol Sci. 2023 Jan 23;24(3):2240. doi: 10.3390/ijms24032240. Int J Mol Sci. 2023. PMID: 36768564 Free PMC article.
-
Integrated Digital Health Solutions in the Management of Growth Disorders in Pediatric Patients Receiving Growth Hormone Therapy: A Retrospective Analysis.Front Endocrinol (Lausanne). 2022 Jun 30;13:882192. doi: 10.3389/fendo.2022.882192. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35846336 Free PMC article.
-
Effect of rhGH treatment on lipidome and brown fat activity in prepuberal small for gestational age children: a pilot study.Sci Rep. 2025 Feb 8;15(1):4710. doi: 10.1038/s41598-025-89546-4. Sci Rep. 2025. PMID: 39922928 Free PMC article.
-
Effect of treatment with growth hormone on body composition and metabolic profile of short children born small for gestational age.Rev Paul Pediatr. 2024 Feb 12;42:e2023073. doi: 10.1590/1984-0462/2024/42/2023073. eCollection 2024. Rev Paul Pediatr. 2024. PMID: 38359318 Free PMC article. Clinical Trial.
References
-
- Lee PA, Chernausek SD, Hokken-Koelega AC, et al. International Small for Gestational Age Advisory Board consensus development conference statement: management of short children born small for gestational age, April 24-October 1, 2001. Pediatrics. 2003;111(6):1253–1261. doi: 10.1542/peds.111.6.1253. - DOI - PubMed
-
- Fujita K, Nagasaka M, Iwatani S, Koda T, Kurokawa D, Yamana K, Nishida K, Taniguchi-Ikeda M, Uchino E, Shirai C, Iijima K, Morioka I. Prevalence of small for gestational age (SGA) and short stature in children born SGA who qualify for growth hormone treatment at 3 years of age: population-based study. Pediatr Int. 2016;58(5):372–376. doi: 10.1111/ped.12859. - DOI - PubMed
-
- Clayton PE, Cianfarani S, Czernichow P, Johannsson G, Rapaport R, Rogol A. Management of the child born small for gestational age through to adulthood: a consensus statement of the International Societies of Pediatric Endocrinology and the Growth Hormone Research Society. J Clin Endocrinol Metab. 2007;92(3):804–810. doi: 10.1210/jc.2006-2017. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
