

The effects of different doses of exercise on pancreatic β-cell function in patients with newly diagnosed type 2 diabetes: study protocol for and rationale behind the "DOSE-EX" multi-arm parallel-group randomised clinical trial
- PMID: 33794975
- PMCID: PMC8017660
- DOI: 10.1186/s13063-021-05207-7
The effects of different doses of exercise on pancreatic β-cell function in patients with newly diagnosed type 2 diabetes: study protocol for and rationale behind the "DOSE-EX" multi-arm parallel-group randomised clinical trial
Abstract
Background: Lifestyle intervention, i.e. diet and physical activity, forms the basis for care of type 2 diabetes (T2D). The current physical activity recommendation for T2D is aerobic training for 150 min/week of moderate to vigorous intensity, supplemented with resistance training 2-3 days/week, with no more than two consecutive days without physical activity. The rationale for the recommendations is based on studies showing a reduction in glycated haemoglobin (HbA1c). This reduction is supposed to be caused by increased insulin sensitivity in muscle and adipose tissue, whereas knowledge about effects on abnormalities in the liver and pancreas are scarce, with the majority of evidence stemming from in vitro and animal studies. The aim of this study is to investigate the role of the volume of exercise training as an adjunct to dietary therapy in order to improve the pancreatic β-cell function in T2D patients less than 7 years from diagnosis. The objective of this protocol for the DOSE-EX trial is to describe the scientific rationale in detail and to provide explicit information about study procedures and planned analyses.
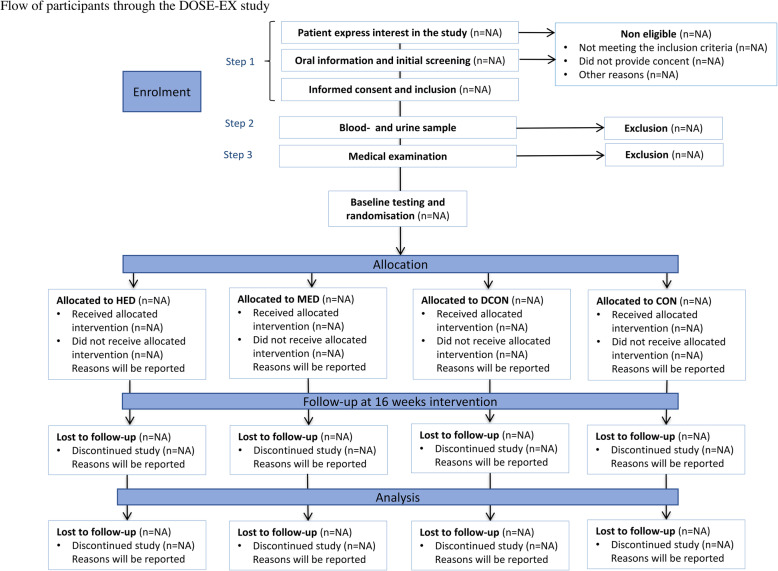
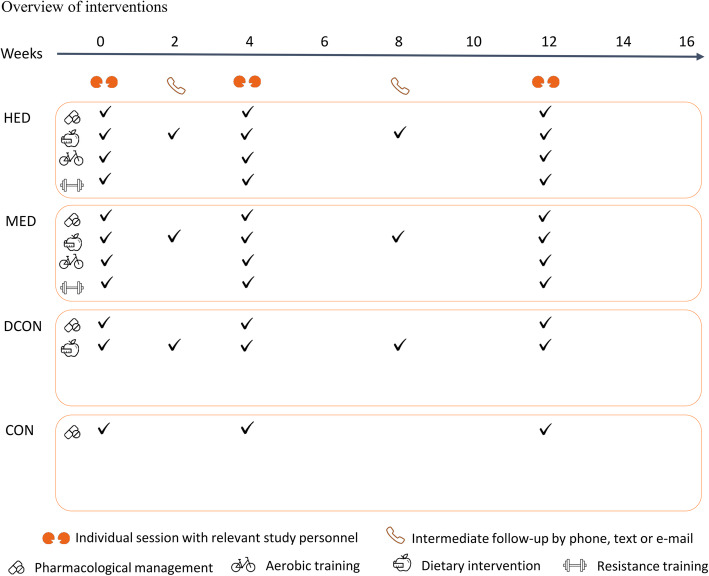
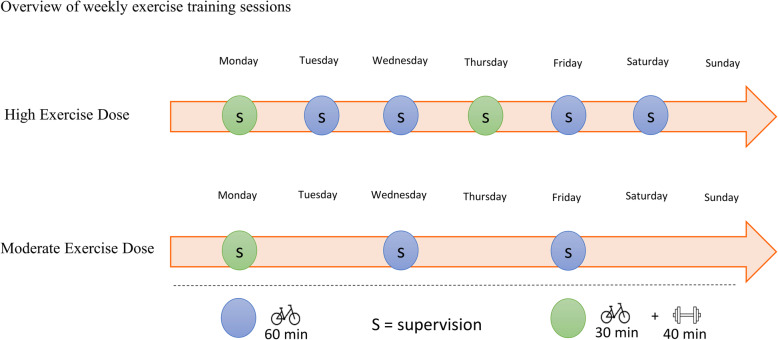
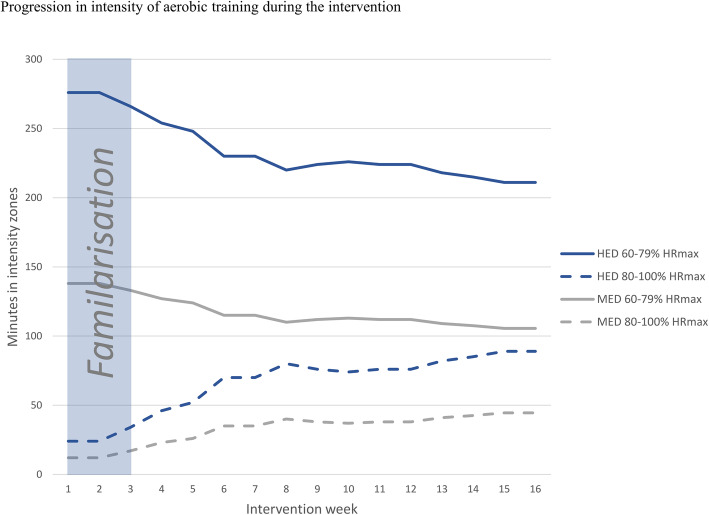
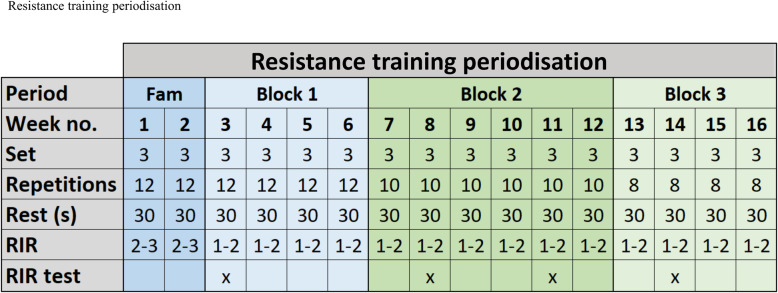
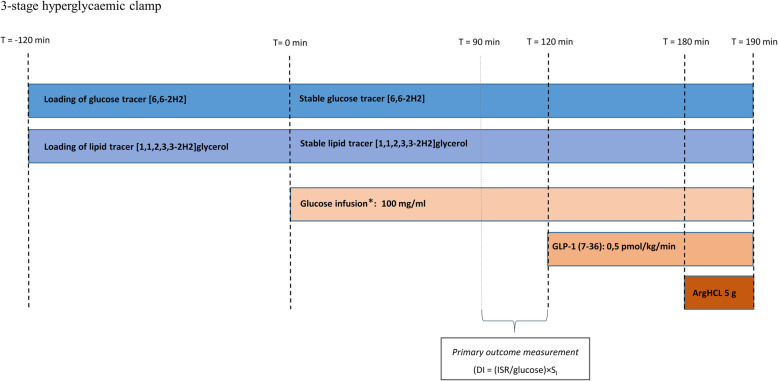
Methods/design: In a parallel-group, 4-arm assessor-blinded randomised clinical trial, 80 patients with T2D will be randomly allocated (1:1:1:1, stratified by sex) to 16 weeks in either of the following groups: (1) no intervention (CON), (2) dietary intervention (DCON), (3) dietary intervention and supervised moderate volume exercise (MED), or (4) dietary intervention and supervised high volume exercise (HED). Enrolment was initiated December 15th, 2018, and will continue until N = 80 or December 1st, 2021. Primary outcome is pancreatic beta-cell function assessed as change in late-phase disposition index (DI) from baseline to follow-up assessed by hyperglycaemic clamp. Secondary outcomes include measures of cardiometabolic risk factors and the effect on subsequent complications related to T2D. The study was approved by The Scientific Ethical Committee at the Capital Region of Denmark (H-18038298).
Trial registration: The Effects of Different Doses of Exercise on Pancreatic β-cell Function in Patients With Newly Diagnosed Type 2 Diabetes (DOSE-EX), NCT03769883, registered 10 December 2018 https://clinicaltrials.gov/ct2/show/NCT03769883 ). Any modification to the protocol, study design, and changes in written participant information will be approved by The Scientific Ethical Committee at the Capital Region of Denmark before effectuation.
Discussion: The data from this study will add knowledge to which volume of exercise training in combination with a dietary intervention is needed to improve β-cell function in T2D. Secondarily, our results will elucidate mechanisms of physical activity mitigating the development of micro- and macrovascular complications correlated with T2D.
Keywords: Exercise; Inflammation; Insulin resistance; Lifestyle intervention; Oxidative stress; Randomised clinical trial; Randomised controlled trial; Type 2 diabetes mellitus; β-cell function.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Colberg SR, Sigal RJ, Fernhall B, Regensteiner JG, Blissmer BJ, Rubin RR, Chasan-Taber L, Albright AL, Braun B. Exercise and type 2 diabetes: the American College of Sports Medicine and the American Diabetes Association: joint position statement. Diabetes Care. 2010;33(12):e147–e167. doi: 10.2337/dc10-9990. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
