

New generation of DNA-based immunotherapy induces a potent immune response and increases the survival in different tumor models
- PMID: 33795383
- PMCID: PMC8021892
- DOI: 10.1136/jitc-2020-001243
New generation of DNA-based immunotherapy induces a potent immune response and increases the survival in different tumor models
Abstract
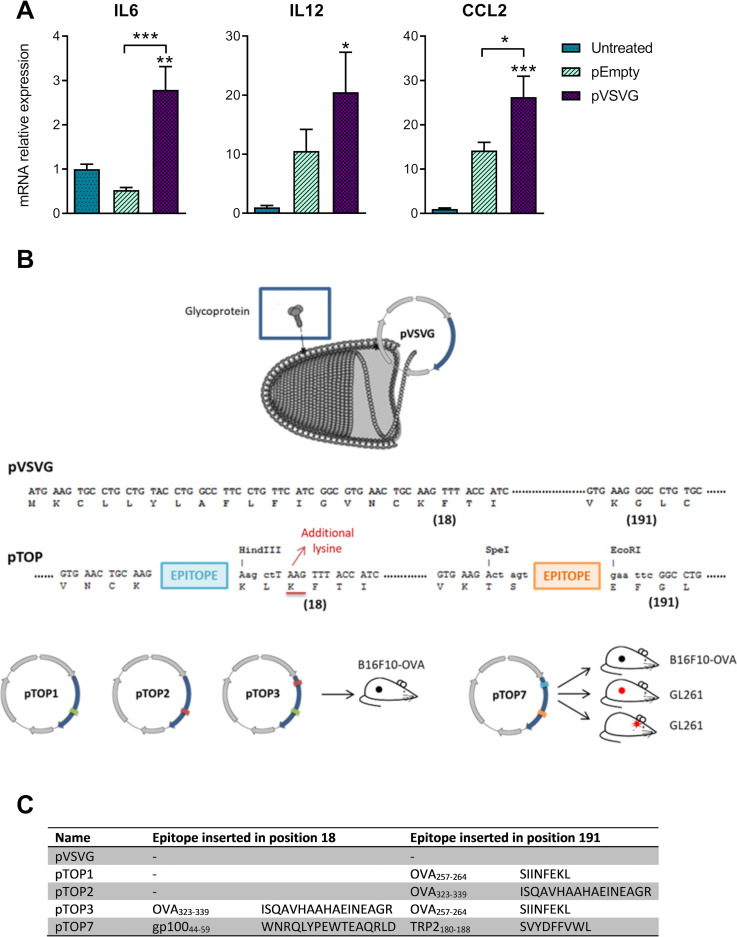
Background: Strategies to increase nucleic acid vaccine immunogenicity are needed to move towards clinical applications in oncology. In this study, we designed a new generation of DNA vaccines, encoding an engineered vesicular stomatitis virus glycoprotein as a carrier of foreign T cell tumor epitopes (plasmid to deliver T cell epitopes, pTOP). We hypothesized that pTOP could activate a more potent response compared with the traditional DNA-based immunotherapies, due to both the innate immune properties of the viral protein and the specific induction of CD4 and CD8 T cells targeting tumor antigens. This could improve the outcome in different tumor models, especially when the DNA-based immunotherapy is combined with a rational therapeutic strategy.
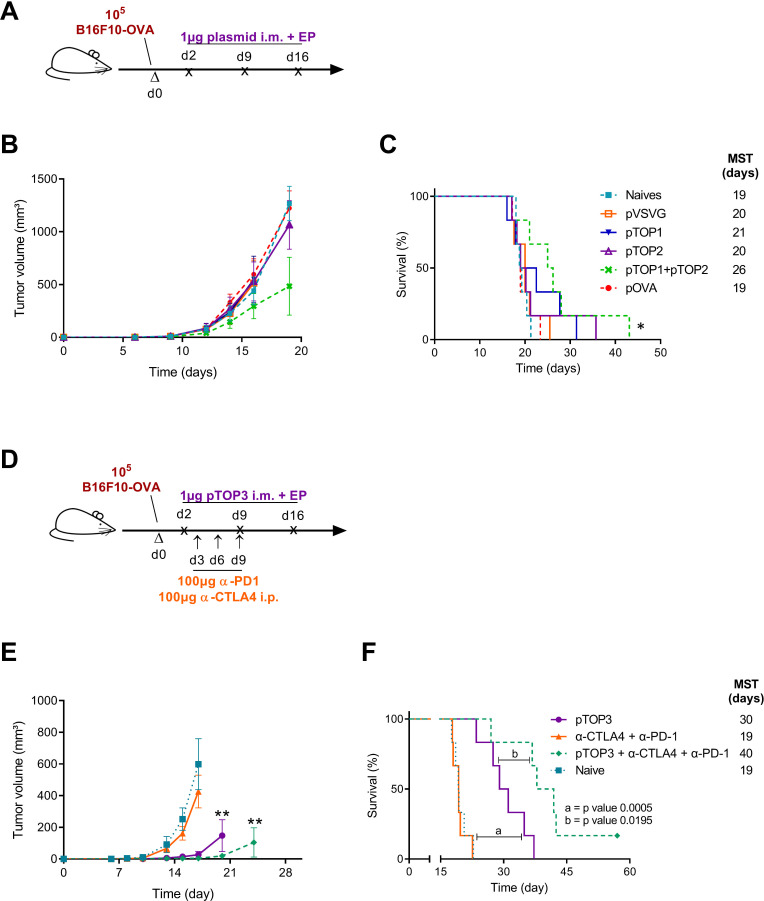
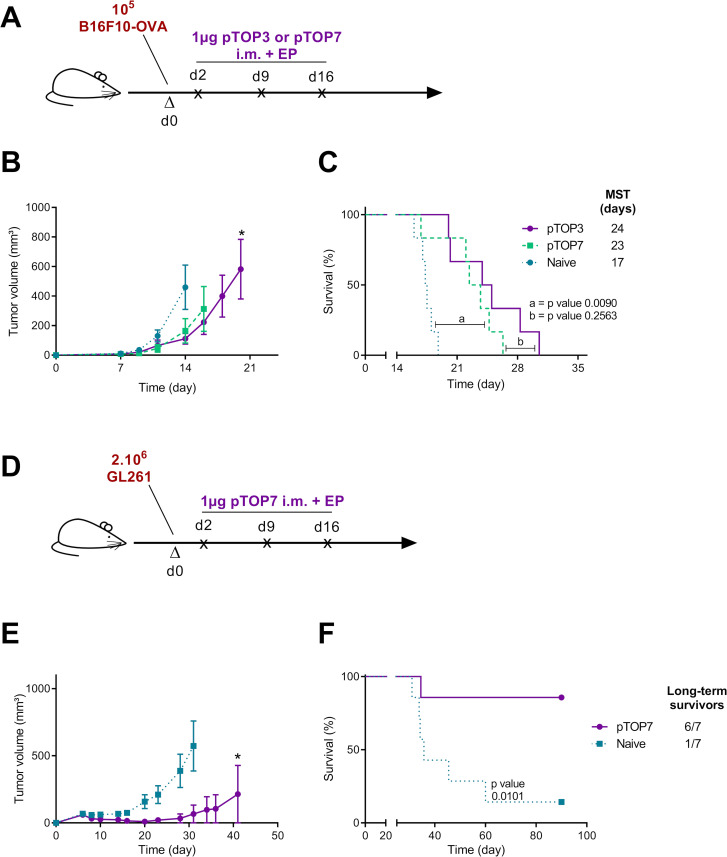
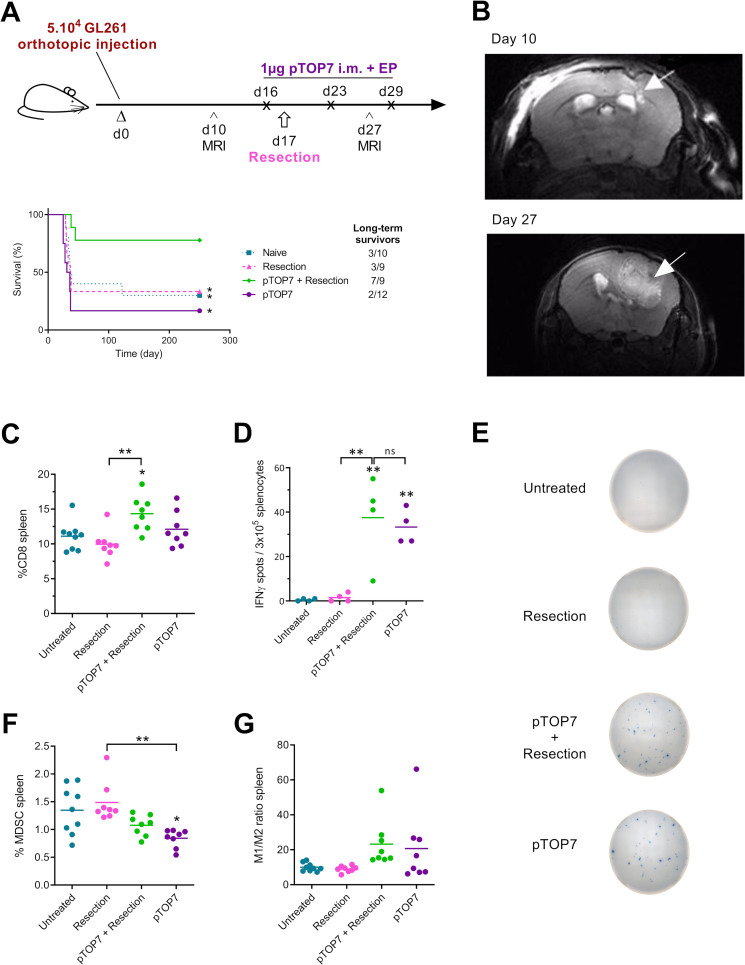
Methods: The ability of pTOP DNA vaccine to activate a specific CD4 and CD8 response and the antitumor efficacy were tested in a B16F10-OVA melanoma (subcutaneous model) and GL261 glioblastoma (subcutaneous and orthotopic models).
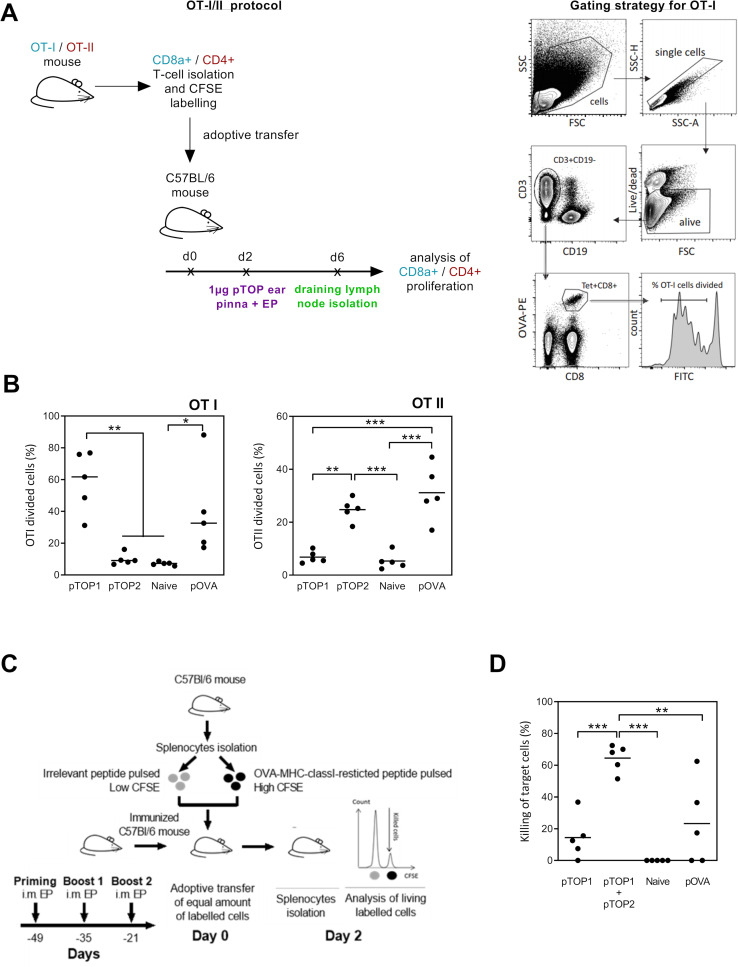
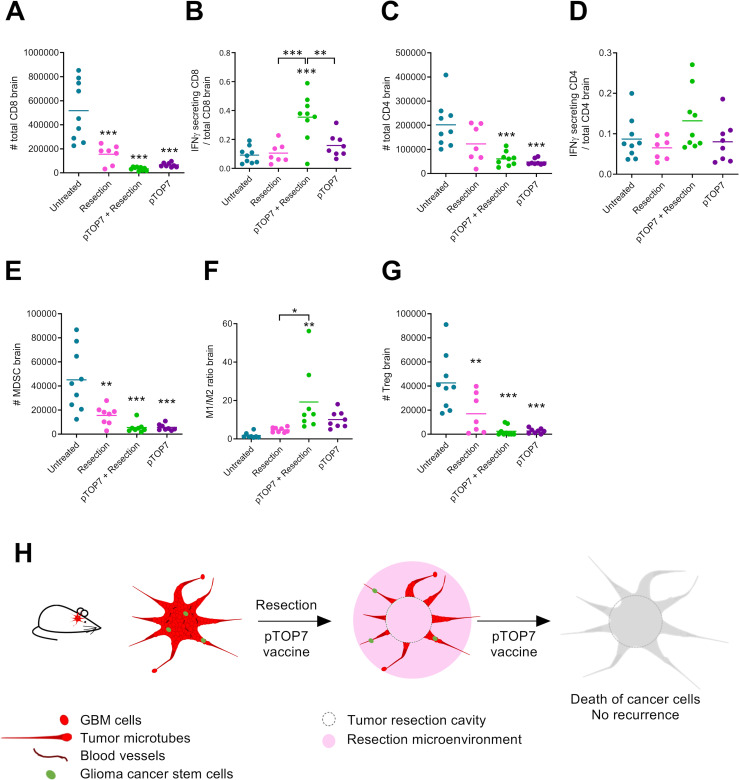
Results: In B16F10-OVA melanoma, pTOP promoted immune recognition by adequate processing of both MHC-I and MHC-II epitopes and had a higher antigen-specific cytotoxic T cell (CTL) killing activity. In a GL261 orthotopic glioblastoma, pTOP immunization prior to tumor debulking resulted in 78% durable remission and long-term survival and induced a decrease of the number of immunosuppressive cells and an increase of immunologically active CTLs in the brain. The combination of pTOP with immune checkpoint blockade or with tumor resection improved the survival of mice bearing, a subcutaneous melanoma or an orthotopic glioblastoma, respectively.
Conclusions: In this work, we showed that pTOP plasmids encoding an engineered vesicular stomatitis virus glycoprotein, and containing various foreign T cell tumor epitopes, successfully triggered innate immunity and effectively promoted immune recognition by adequate processing of both MHC-I and MHC-II epitopes. These results highlight the potential of DNA-based immunotherapies coding for viral proteins to induce potent and specific antitumor responses.
Keywords: active; adaptive immunity; antigens; cellular; immunity; immunotherapy; vaccination.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: GV, LL and VP are coapplicants of a patent: 'Modified VSV-G and vaccines thereof', PCT/EP2017/073119. GV, AL, CB and VP are coapplicants of a patent: 'Modified vesicular stomatitis virus glycoprotein and uses thereof for the treatment of brain tumors', EP19199334.4. Both patents are pending.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials