

Tranexamic acid for acute intracerebral haemorrhage growth based on imaging assessment (TRAIGE): a multicentre, randomised, placebo-controlled trial
- PMID: 33795488
- PMCID: PMC8258050
- DOI: 10.1136/svn-2021-000942
Tranexamic acid for acute intracerebral haemorrhage growth based on imaging assessment (TRAIGE): a multicentre, randomised, placebo-controlled trial
Abstract
Background: Studies show tranexamic acid can reduce the risk of death and early neurological deterioration after intracranial haemorrhage. We aimed to assess whether tranexamic acid reduces haematoma expansion and improves outcome in intracerebral haemorrhage patients susceptible to haemorrhage expansion.
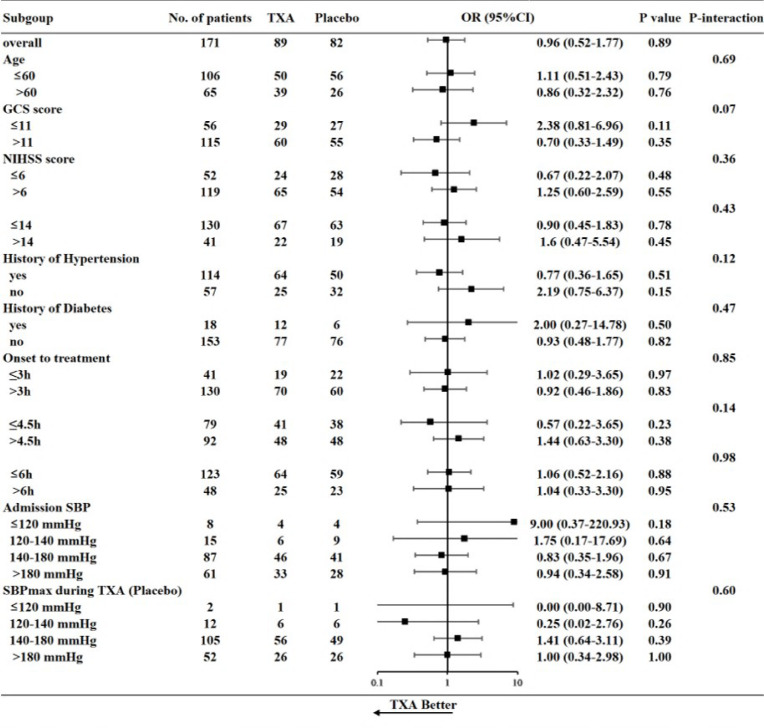
Methods: We did a prospective, double-blind, randomised, placebo-controlled trial at 10 stroke centres in China. Acute supratentorial intracerebral haemorrhage patients were eligible if they had indication of haemorrhage expansion on admission imaging (eg, spot sign, black hole sign or blend sign), and were treatable within 8 hours of symptom onset. Patients were randomly assigned (1:1) to receive either tranexamic acid or a matching placebo. The primary outcome was intracerebral haematoma growth (>33% relative or >6 mL absolute) at 24 hours. Clinical outcomes were assessed at 90 days.
Results: Of the 171 included patients, 124 (72.5%) were male, and the mean age was 55.9±11.6 years. 89 patients received tranexamic acid and 82 received placebo. The primary outcome did not differ significantly between the groups: 36 (40.4%) patients in the tranexamic acid group and 34 (41.5%) patients in the placebo group had intracranial haemorrhage growth (OR 0.96, 95% CI 0.52 to 1.77, p=0.89). The proportion of death was lower in the tranexamic acid treatment group than placebo group (8.1% vs 10.0%), but there were no significant differences in secondary outcomes including absolute intracranial haemorrhage growth, death and dependency.
Conclusions: Among patients susceptible to haemorrhage expansion treated within 8 hours of stroke onset, tranexamic acid did not significantly prevent intracerebral haemorrhage growth. Larger studies are needed to assess safety and efficacy of tranexamic acid in intracerebral haemorrhage patients.
Keywords: CT; CT angiography; drug; hemorrhage; stroke.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources