

Improving estimation of Parkinson's disease risk-the enhanced PREDICT-PD algorithm
- PMID: 33795693
- PMCID: PMC8017005
- DOI: 10.1038/s41531-021-00176-9
Improving estimation of Parkinson's disease risk-the enhanced PREDICT-PD algorithm
Abstract
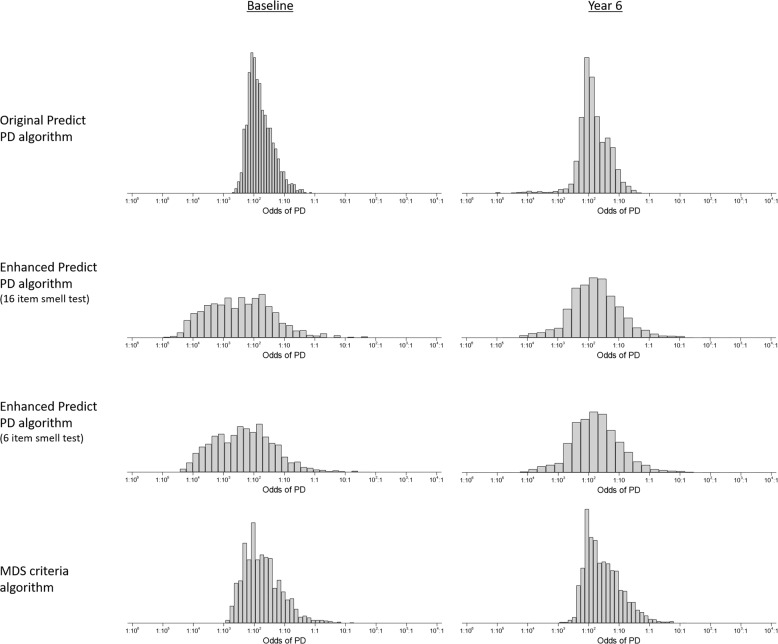
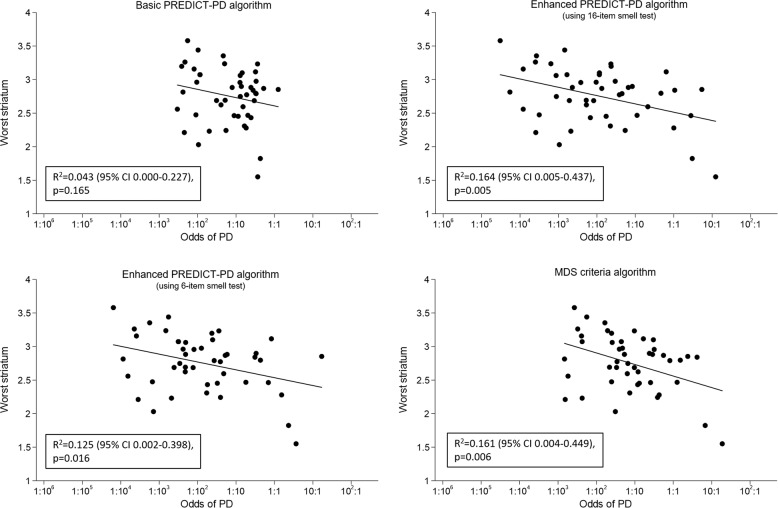
We previously reported a basic algorithm to identify the risk of Parkinson's disease (PD) using published data on risk factors and prodromal features. Using this algorithm, the PREDICT-PD study identified individuals at increased risk of PD and used tapping speed, hyposmia and REM sleep behaviour disorder (RBD) as "intermediate" markers of prodromal PD in the absence of sufficient incident cases. We have now developed and tested an enhanced algorithm which incorporates the intermediate markers into the risk model. Risk estimates were compared using the enhanced and the basic algorithm in members of the PREDICT-PD pilot cohort. The enhanced PREDICT-PD algorithm yielded a much greater range of risk estimates than the basic algorithm (93-609-fold difference between the 10th and 90th centiles vs 10-13-fold respectively). There was a greater increase in the risk of PD with increasing risk scores for the enhanced algorithm than for the basic algorithm (hazard ratios per one standard deviation increase in log risk of 2.75 [95% CI 1.68-4.50; p < 0.001] versus 1.47 [95% CI 0.86-2.51; p = 0.16] respectively). Estimates from the enhanced algorithm also correlated more closely with subclinical striatal DaT-SPECT dopamine depletion (R2 = 0.164, p = 0.005 vs R2 = 0.043, p = 0.17). Incorporating the previous intermediate markers of prodromal PD and using likelihood ratios improved the accuracy of the PREDICT-PD prediction algorithm.
Conflict of interest statement
Alastair Noyce—Dr. Noyce is funded by the Barts Charity. Dr. Noyce reports additional grants from Parkinson’s UK, Virginia Keiley benefaction, UCL-Movement Disorders Centre, grants and non-financial support from GE Healthcare, and personal fees from LEK, Guidepoint, Profile, Roche, Biogen, Bial and Britannia, outside the submitted work. Anette Schrag—Prof Schrag is employed by University College London and NHS National Institute for Health Research UCL Biomedical Research Centre. She has received grants from the European Commission, Parkinson’s UK, GE Healthcare, Economic and Social Research Council (ESRC), International Parkinson’s and Movement Disorders Society, University College London, National Institute of Health (NIHR), National Institute for Health Research ULCH Biomedical Research Centre; honoraria from Health Advances; advisory board fees from GE Healthcare, Roche, Biogen, Bial; and royalties from Oxford University Press for Rating Scales in PD, University College London Business. Andrew Lees is funded by the Reta Lila Weston Institute of Neurological Studies, University College London, Institute of Neurology and reports consultancies from: Britannia Pharmaceuticals and BIAL Portela. He also reports grants and/or research support from the Frances and Renee Hock Fund, and honoraria from Britannia, Profle Pharma, UCB, Roche, BIAL, STADA Nordic, Nordiclnfu Care, and NeuroDerm. Stephen Auger—Dr Auger is employed by Health Education England. Jonathan Bestwick, Cristina Simonet, Richard Rees, Daniel Rack, Jack Cuzick, Gavin Giovannoni and Mark Jitlal report no relevant disclosures.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
