

Hospitalization rates for complications due to systemic therapy in the United States
- PMID: 33795827
- PMCID: PMC8016938
- DOI: 10.1038/s41598-021-86911-x
Hospitalization rates for complications due to systemic therapy in the United States
Abstract
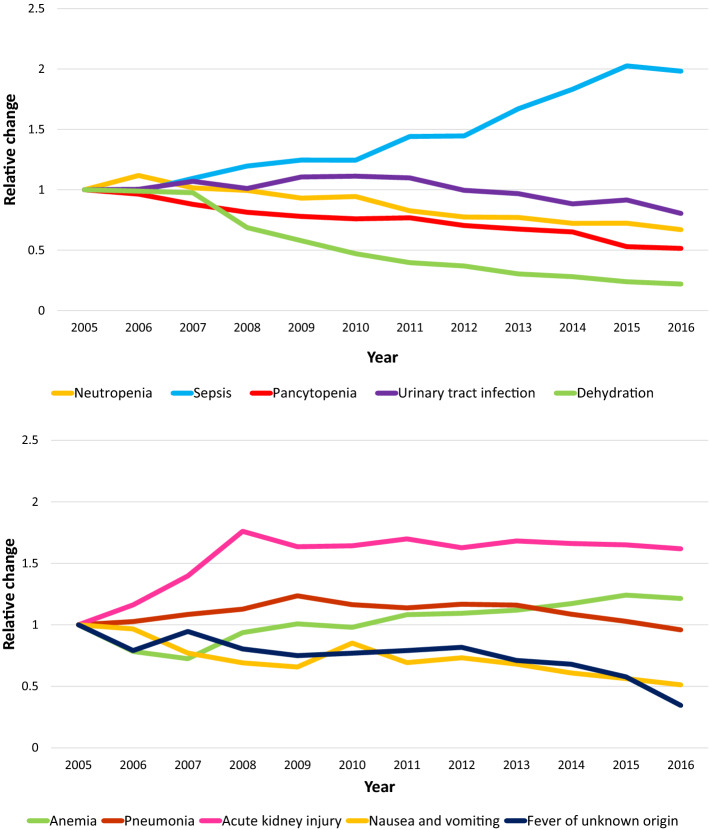
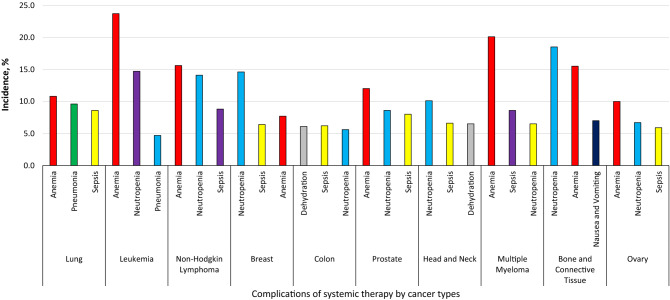
The aim of this study was to estimate the trends and burdens associated with systemic therapy-related hospitalizations, using nationally representative data. National Inpatient Sample data from 2005 to 2016 was used to identify systemic therapy-related complications using ICD-9 and ICD-10 external causes-of-injury codes. The primary outcome was hospitalization rates, while secondary outcomes were cost and in-hospital mortality. Overall, there were 443,222,223 hospitalizations during the study period, of which 2,419,722 were due to complications of systemic therapy. The average annual percentage change of these hospitalizations was 8.1%, compared to - 0.5% for general hospitalizations. The three most common causes for hospitalization were anemia (12.8%), neutropenia (10.8%), and sepsis (7.8%). Hospitalization rates had the highest relative increases for sepsis (1.9-fold) and acute kidney injury (1.6-fold), and the highest relative decrease for dehydration (0.21-fold) and fever of unknown origin (0.35-fold). Complications with the highest total charges were anemia ($4.6 billion), neutropenia ($3.0 billion), and sepsis ($2.5 billion). The leading causes of in-hospital mortality associated with systemic therapy were sepsis (15.8%), pneumonia (7.6%), and acute kidney injury (7.0%). Promoting initiatives such as rule OP-35, improving access to and providing coordinated care, developing systems leading to early identification and management of symptoms, and expanding urgent care access, can decrease these hospitalizations and the burden they carry on the healthcare system.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Cancer Statistics. https://www.cancer.gov/about-cancer/understanding/statistics.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
