

Complications and Comorbidities of Acromegaly-Retrospective Study in Polish Center
- PMID: 33796075
- PMCID: PMC8009182
- DOI: 10.3389/fendo.2021.642131
Complications and Comorbidities of Acromegaly-Retrospective Study in Polish Center
Abstract
Introduction: In acromegaly, chronic exposure to impaired GH and IGF-I levels leads to the development of typical acromegaly symptoms, and multiple systemic complications as cardiovascular, metabolic, respiratory, endocrine, and bone disorders. Acromegaly comorbidities contribute to decreased life quality and premature mortality. The aim of our study was to assess the frequency of acromegaly complications and to evaluate diagnostic methods performed toward recognition of them.
Materials and methods: It was a retrospective study and we analyzed data of 179 patients hospitalized in the Department of Endocrinology, Diabetes and Isotope Therapy in Wroclaw Medical University (Poland) in 1976 to 2018 to create a database for statistical analysis.
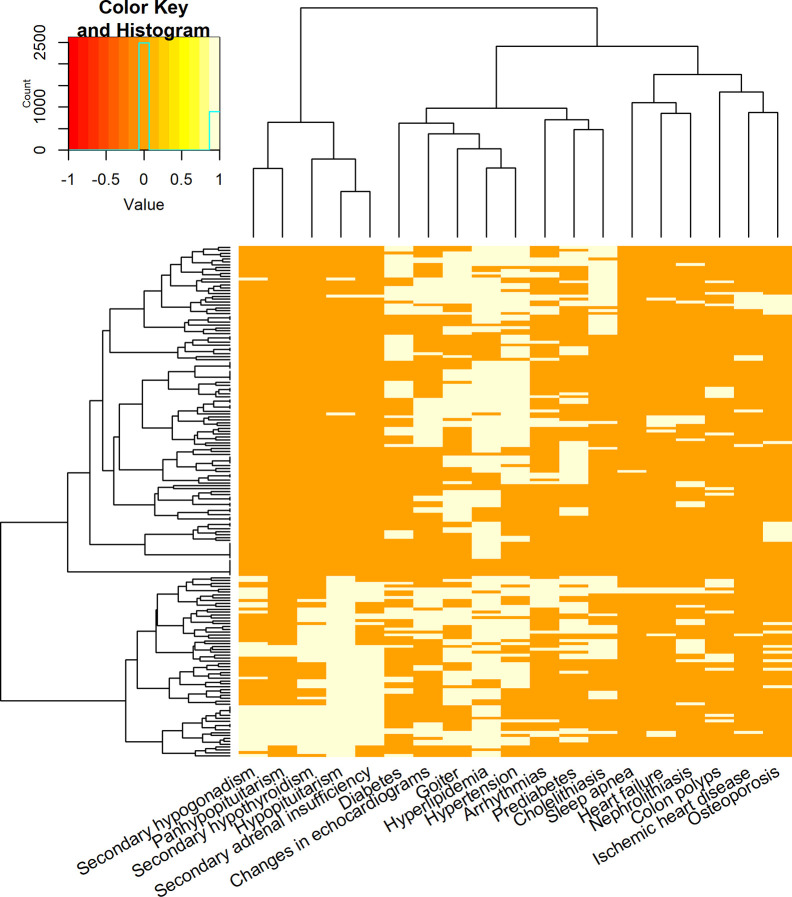
Results: The study group comprised of 119 women (66%) and 60 men (34%). The median age of acromegaly diagnosis was 50.5 years old for women (age range 20-78) and 46 for men (range 24-76). Metabolic disorders (hyperlipidemia, diabetes, and prediabetes) were the most frequently diagnosed complications in our study, followed by cardiovascular diseases and endocrine disorders (goiter, pituitary insufficiency, osteoporosis). BP measurement, ECG, lipid profile, fasting glucose or OGTT were performed the most often, while colonoscopy and echocardiogram were the least frequent.
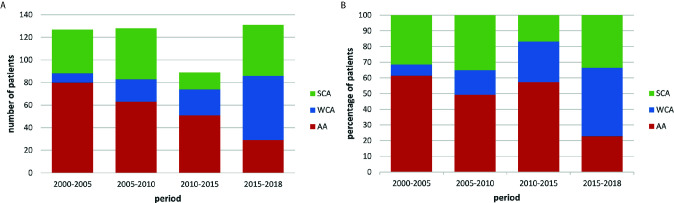
Conclusions: In our population we observed female predominance. We revealed a decrease in the number of patients with active acromegaly and an increase in the number of well-controlled patients. More than 50% of patients demonstrated a coexistence of cardiac, metabolic and endocrine disturbances and only 5% of patients did not suffer from any disease from those main groups.
Keywords: GH; IGF-I; acromegaly; comorbidity; complication; pituitary adenoma.
Copyright © 2021 Rolla, Jawiarczyk-Przybyłowska, Halupczok-Żyła, Kałużny, Konopka, Błoniecka, Zieliński and Bolanowski.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The effects of long-term growth hormone and insulin-like growth factor-1 exposure on the development of cardiovascular, cerebrovascular and metabolic co-morbidities in treated patients with acromegaly.Clin Endocrinol (Oxf). 2011 Aug;75(2):220-5. doi: 10.1111/j.1365-2265.2011.04019.x. Clin Endocrinol (Oxf). 2011. PMID: 21521288
-
Prevalence of thyroid diseases in patients with acromegaly: results of an Italian multi-center study.J Endocrinol Invest. 2002 Mar;25(3):240-5. doi: 10.1007/BF03343997. J Endocrinol Invest. 2002. PMID: 11936466
-
Long-term biochemical status and disease-related morbidity in 53 postoperative patients with acromegaly.J Clin Endocrinol Metab. 2004 Feb;89(2):658-61. doi: 10.1210/jc.2003-030915. J Clin Endocrinol Metab. 2004. PMID: 14764777
-
[Acromegaly and it's cardiovascular implications].Rev Med Inst Mex Seguro Soc. 2021 Feb 2;59(1):73-80. doi: 10.24875/RMIMSS.M21000054. Rev Med Inst Mex Seguro Soc. 2021. PMID: 33667046 Review. Spanish.
-
Hormonal diagnosis of GH hypersecretory states.J Endocrinol Invest. 2003;26(10 Suppl):27-35. J Endocrinol Invest. 2003. PMID: 15497657 Review.
Cited by
-
Acromegaly Caused by Ectopic Growth Hormone Releasing Hormone Secretion: A Review.Front Endocrinol (Lausanne). 2022 Jun 9;13:867965. doi: 10.3389/fendo.2022.867965. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35757397 Free PMC article. Review.
-
Diabetic Ketoacidosis in Undiagnosed Acromegaly: A Case Report and Literature Review.Kans J Med. 2022 Feb 9;15(1):70-72. doi: 10.17161/kjm.vol15.15881. eCollection 2022. Kans J Med. 2022. PMID: 35371390 Free PMC article. No abstract available.
-
The Relationship between the Burden of Acromegaly, Associated Comorbidities, Complications and Disease Status.J Clin Med. 2023 Sep 30;12(19):6309. doi: 10.3390/jcm12196309. J Clin Med. 2023. PMID: 37834952 Free PMC article.
-
Osteosarcopenia in acromegaly: reduced muscle quality and increased vertebral fat deposition.J Endocrinol Invest. 2023 Dec;46(12):2573-2582. doi: 10.1007/s40618-023-02114-3. Epub 2023 May 22. J Endocrinol Invest. 2023. PMID: 37212954
-
Lipoprotein alterations in endocrine disorders - a review of the recent developments in the field.Front Endocrinol (Lausanne). 2024 Apr 2;15:1354098. doi: 10.3389/fendo.2024.1354098. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38628593 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous