

Rates of Concomitant Meniscal Tears in Pediatric Patients With Anterior Cruciate Ligament Injuries Increase With Age and Body Mass Index
- PMID: 33796585
- PMCID: PMC7968031
- DOI: 10.1177/2325967120986565
Rates of Concomitant Meniscal Tears in Pediatric Patients With Anterior Cruciate Ligament Injuries Increase With Age and Body Mass Index
Abstract
Background: Anterior cruciate ligament (ACL) tears are frequently associated with meniscal injury. Risk factors for concomitant meniscal injuries have been studied in the adult population but less so in pediatric patients.
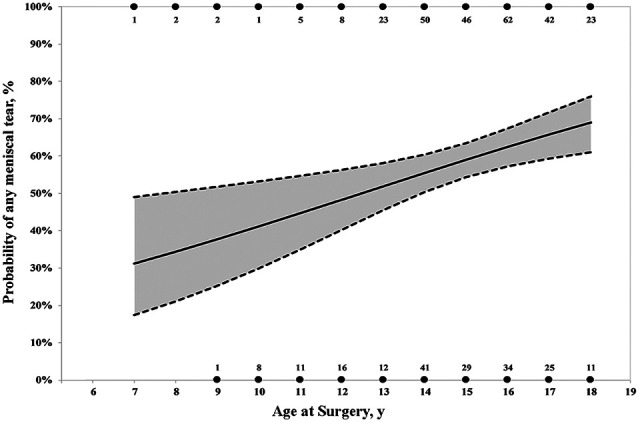
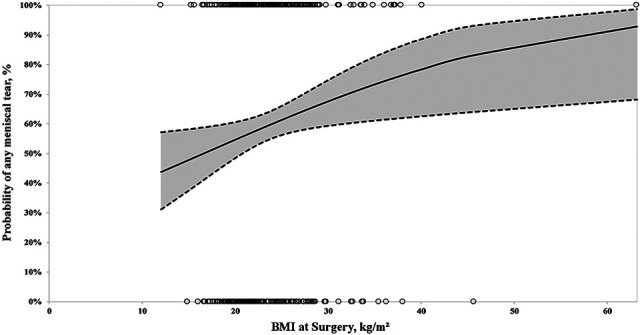
Purpose: To evaluate the relationship between age and body mass index (BMI) and the presence of a concomitant meniscal tear at the time of ACL reconstruction (ACLR) in pediatric patients.
Study design: Case-control study; Level of evidence, 3.
Methods: A single-institution retrospective review was performed of patients aged <19 years who underwent primary ACLR over a 3.5-year period. Revision ACLR and multiligament knee reconstructions were excluded. Logistic regression was used to identify risk factors associated with having a meniscal tear at the time of surgery. Subgroup analysis was performed for medial and lateral meniscal tears.
Results: Included in this study were 453 patients (230 males, 223 females; median age, 15 years). Of these, 265 patients (58%) had a meniscal tear, including 150 isolated lateral meniscal tears, 53 isolated medial meniscal tears, and 62 patients with both lateral and medial meniscal tears. Median time from injury to surgery was 48 days. For every 1-year increase in age, there was a 16% increase in the adjusted odds of having any meniscal tear (odds ratio [OR], 1.16; 95% confidence interval [CI], 1.05-1.27; P = .002), with a 20% increase in the odds of having a medial meniscal tear (OR, 1.20; 95% CI, 1.07-1.35; P = .002) and a 16% increase in the odds of having a lateral meniscal tear (OR, 1.16; 95% CI, 1.05-1.27; P = .003). For every 2-point increase in BMI, there was a 12% increase in the odds of having any meniscal tear (OR, 1.12; 95% CI, 1.02-1.22; P = .016) and a 10% increase in the odds of having a lateral meniscal tear (OR, 1.10; 95% CI, 1.01-1.19; P = .028).
Conclusion: Pediatric patients undergoing ACLR had a 58% incidence of concomitant meniscal pathology. Increasing age and BMI were independent risk factors for these injuries, while no association was found between time to surgery and meniscal pathology.
Keywords: ACL tear; BMI; meniscus tear; pediatric; risk factors.
© The Author(s) 2021.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: C.A.P. has received research funding from DJO and OrthoPediatrics and education payments from Smith & Nephew and Arthrex. M.A.C. has received research funding from DJO and OrthoPediatrics and education payments Smith & Nephew. M.T.B. has received research support from OrthoPediatrics and education payments and nonconsulting fees from Arthrex. S.C.W. has received research support from OrthoPediatrics, education payments from Arthrex, and nonconsulting fees from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
Similar articles
-
Increased Lateral Posterior Tibial Slope Is Associated With a Greater Rate of Lateral Meniscal Injury in Acute Noncontact Anterior Cruciate Ligament Ruptures.Arthroscopy. 2025 Mar 15:S0749-8063(25)00167-7. doi: 10.1016/j.arthro.2025.03.011. Online ahead of print. Arthroscopy. 2025. PMID: 40090529
-
Correlation of meniscal and articular cartilage injuries in children and adolescents with timing of anterior cruciate ligament reconstruction.Am J Sports Med. 2015 Feb;43(2):275-81. doi: 10.1177/0363546514559912. Epub 2014 Dec 12. Am J Sports Med. 2015. PMID: 25497145
-
Delayed ACL Reconstruction in Patients ≥40 Years of Age Is Associated With Increased Risk of Medial Meniscal Injury at 1 Year.Am J Sports Med. 2019 Mar;47(3):584-589. doi: 10.1177/0363546518817749. Epub 2019 Jan 9. Am J Sports Med. 2019. PMID: 30624961
-
Associated injuries in pediatric and adolescent anterior cruciate ligament tears: does a delay in treatment increase the risk of meniscal tear?Arthroscopy. 2002 Nov-Dec;18(9):955-9. doi: 10.1053/jars.2002.36114. Arthroscopy. 2002. PMID: 12426537 Review.
-
Early Operative Versus Delayed Operative Versus Nonoperative Treatment of Pediatric and Adolescent Anterior Cruciate Ligament Injuries: A Systematic Review and Meta-analysis.Am J Sports Med. 2021 Dec;49(14):4008-4017. doi: 10.1177/0363546521990817. Epub 2021 Mar 15. Am J Sports Med. 2021. PMID: 33720764
Cited by
-
Low meniscus reoperation rates following meniscus repair during anterior cruciate ligament reconstruction in Turkey: an in-depth national analysis of 8-years.BMC Musculoskelet Disord. 2024 Jul 17;25(1):554. doi: 10.1186/s12891-024-07662-0. BMC Musculoskelet Disord. 2024. PMID: 39020339 Free PMC article.
-
Anterior Cruciate Ligament Injury in Association With Other Knee Injuries in King Abdulaziz University Hospital, Saudi Arabia.Cureus. 2020 Sep 4;12(9):e10240. doi: 10.7759/cureus.10240. Cureus. 2020. PMID: 33042680 Free PMC article.
-
Lateral Meniscal Oblique Radial Tears Were Observed Concomitantly With Anterior Cruciate Ligament Tears in 6% of Pediatric Patients Undergoing Anterior Cruciate Ligament Reconstruction.Arthrosc Sports Med Rehabil. 2024 Sep 26;7(1):101012. doi: 10.1016/j.asmr.2024.101012. eCollection 2025 Feb. Arthrosc Sports Med Rehabil. 2024. PMID: 40041834 Free PMC article.
-
Deficits in Dynamic Balance and Hop Performance Following ACL Reconstruction Are Not Dependent on Meniscal Injury History.Int J Sports Phys Ther. 2022 Dec 1;17(7):1298-1306. doi: 10.26603/001c.55542. eCollection 2022. Int J Sports Phys Ther. 2022. PMID: 36518839 Free PMC article.
-
Medial meniscus tears are most prevalent in type I ACL tears, while type I ACL tears only account for 8% of all ACL tears.Knee Surg Sports Traumatol Arthrosc. 2023 Jun;31(6):2349-2357. doi: 10.1007/s00167-022-07068-2. Epub 2022 Jul 17. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 35842857
References
-
- Ahn JH, Bae TS, Kang KS, Kang SY, Lee SH. Longitudinal tear of the medial meniscus posterior horn in the anterior cruciate ligament-deficient knee significantly influences anterior stability. Am J Sports Med. 2011;39(10):2187–2193. - PubMed
-
- Anderson AF, Anderson CN. Correlation of meniscal and articular cartilage injuries in children and adolescents with timing of anterior cruciate ligament reconstruction. Am J Sports Med. 2015;43(2):275–281. - PubMed
-
- Bellabarba C, Bush-Joseph CA, Bach BR, Jr. Patterns of meniscal injury in the anterior cruciate-deficient knee: a review of the literature. Am J Orthop (Belle Mead NJ). 1997;26(1):18–23. - PubMed
-
- Brambilla L, Pulici L, Carimati G, et al. Prevalence of associated lesions in anterior cruciate ligament reconstruction: correlation with surgical timing and with patient age, sex, and body mass index. Am J Sports Med. 2015;43(12):2966–2973. - PubMed
-
- Chhadia AM, Inacio MC, Maletis GB, et al. Are meniscus and cartilage injuries related to time to anterior cruciate ligament reconstruction? Am J Sports Med. 2011;39(9):1894–1899. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
