

The diagnostic value of the neurological examination in coma of unknown etiology
- PMID: 33796895
- PMCID: PMC8463407
- DOI: 10.1007/s00415-021-10527-4
The diagnostic value of the neurological examination in coma of unknown etiology
Abstract
Background: Identifying the cause of non-traumatic coma in the emergency department is challenging. The clinical neurological examination is the most readily available tool to detect focal neurological deficits as indicators for cerebral causes of coma. Previously proposed clinical pathways have granted the interpretation of clinical findings a pivotal role in the diagnostic work-up. We aimed to identify the actual diagnostic reliability of the neurological examination with regard to identifying acute brain damage.
Methods: Eight hundred and fifty-three patients with coma of unknown etiology (CUE) were examined neurologically in the emergency department following a predefined routine. Coma-explaining pathologies were identified retrospectively and grouped into primary brain pathology with proof of acute brain damage and other causes without proof of acute structural pathology. Sensitivity, specificity and percentage of correct predictions of different examination protocols were calculated using contingency tables and binary logistic regression models.
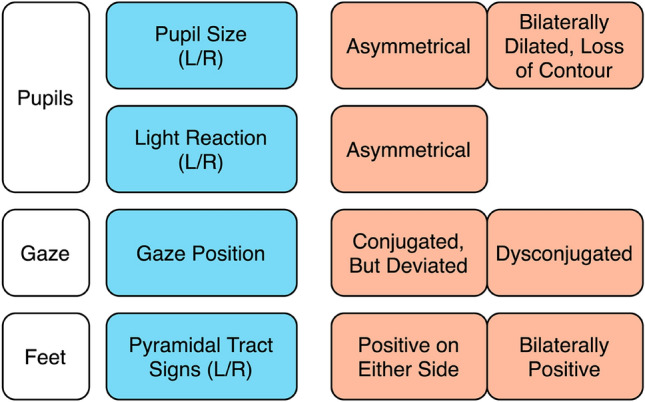
Results: The full neurological examination was 74% sensitive and 60% specific to detect acute structural brain damage underlying CUE. Sensitivity and specificity were higher in non-sedated patients (87/61%) compared to sedated patients (64%/59%). A shortened four-item examination protocol focusing on pupils, gaze and pyramidal tract signs was only slightly less sensitive (67%) and more specific (65%).
Conclusions: Due to limited diagnostic reliability of the physical examination, the absence of focal neurological signs in acutely comatose patients should not defer from a complete work-up including brain imaging. In an emergency, a concise neurological examination should thus serve as one part of a multimodal diagnostic approach to CUE.
Keywords: Coma; Critical pathways; Neurologic examination; Neurological emergencies; Reproducibility of results.
© 2021. The Author(s).
Conflict of interest statement
There are no conflicts of interest to declare regarding funding/sponsoring of this manuscript from any of the authors.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
