

Choice of CTO scores to predict procedural success in clinical practice. A comparison of 4 different CTO PCI scores in a comprehensive national registry including expert and learning CTO operators
- PMID: 33798205
- PMCID: PMC8018648
- DOI: 10.1371/journal.pone.0245898
Choice of CTO scores to predict procedural success in clinical practice. A comparison of 4 different CTO PCI scores in a comprehensive national registry including expert and learning CTO operators
Abstract
Background: We aimed to compare the performance of the recent CASTLE score to J-CTO, CL and PROGRESS CTO scores in a comprehensive database of percutaneous coronary intervention of chronic total occlusion procedures.
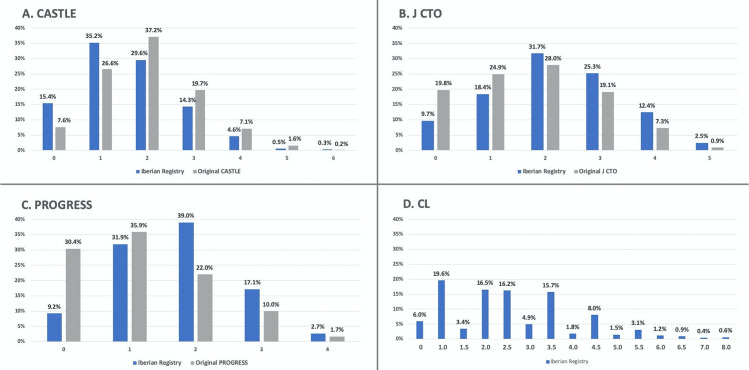
Methods: Scores were calculated using raw data from 1,342 chronic total occlusion procedures included in REBECO Registry that includes learning and expert operators. Calibration, discrimination and reclassification were evaluated and compared.
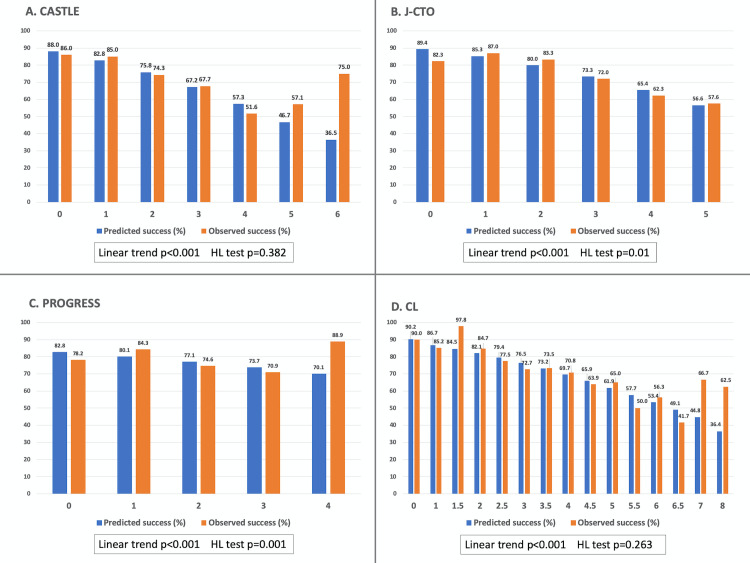
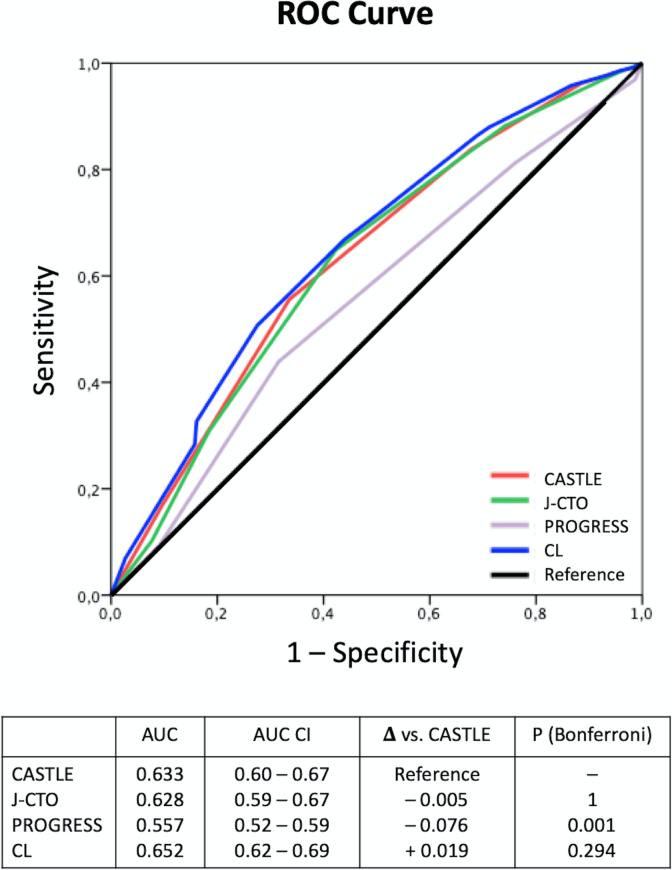
Results: Mean score values were: CASTLE 1.60±1.10, J-CTO 2.15±1.24, PROGRESS 1.68±0.94 and CL 2.52±1.52 points. The overall percutaneous coronary intervention success rate was 77.8%. Calibration was good for CASTLE and CL, but not for J-CTO or PROGRESS scores. Discrimination: the area under the curve (AUC) of CASTLE (0.633) was significantly higher than PROGRESS (0.557) and similar to J-CTO (0.628) and CL (0.652). Reclassification: CASTLE, as assessed by integrated discrimination improvement, was superior to PROGRESS (integrated discrimination improvement +0.036, p<0.001), similar to J-CTO and slightly inferior to CL score (- 0.011, p = 0.004). Regarding net reclassification improvement, CASTLE reclassified better than PROGRESS (overall continuous net reclassification improvement 0.379, p<0.001) in roughly 20% of cases.
Conclusion: Procedural percutaneous coronary intervention difficulty is not consistently depicted by available chronic total occlusion scores and is influenced by the characteristics of each chronic total occlusion cohort. In our study population, including expert and learning operators, the CASTLE score had slightly better overall performance along with CL score. However, we found only intermediate performance in the c-statistic predicting chronic total occlusion success among all scores.
Conflict of interest statement
Abbott provided an unrestricted grant to support the Registry and this publication’s fees. There are no patents, products in development or marketed products associated with this research to declare. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Galassi A, Werner G, Boukhris M, Azzalini L, Mashayekhi K, Carlino M, et al. Percutaneous recanalisation of chronic total occlusions: 2019 consensus document from the EuroCTO Club [Internet]. EuroIntervention. [citado 10 de agosto de 2019]. Disponible en: https://eurointervention.pcronline.com/article/percutaneous-recanalizati... - PubMed
-
- Neumann F-J, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. EuroIntervention J Eur Collab Work Group Interv Cardiol Eur Soc Cardiol. 20 de Febrero de 2019;14(14):1435–534. - PubMed
-
- Morino Y, Abe M, Morimoto T, Kimura T, Hayashi Y, Muramatsu T, et al. Predicting Successful Guidewire Crossing Through Chronic Total Occlusion of Native Coronary Lesions Within 30 Minutes: The J-CTO (Multicenter CTO Registry in Japan) Score as a Difficulty Grading and Time Assessment Tool. JACC Cardiovasc Interv. 1 de Febrero de 2011;4(2):213–21. 10.1016/j.jcin.2010.09.024 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
