

A catalog of GWAS fine-mapping efforts in autoimmune disease
- PMID: 33798443
- PMCID: PMC8059376
- DOI: 10.1016/j.ajhg.2021.03.009
A catalog of GWAS fine-mapping efforts in autoimmune disease
Abstract
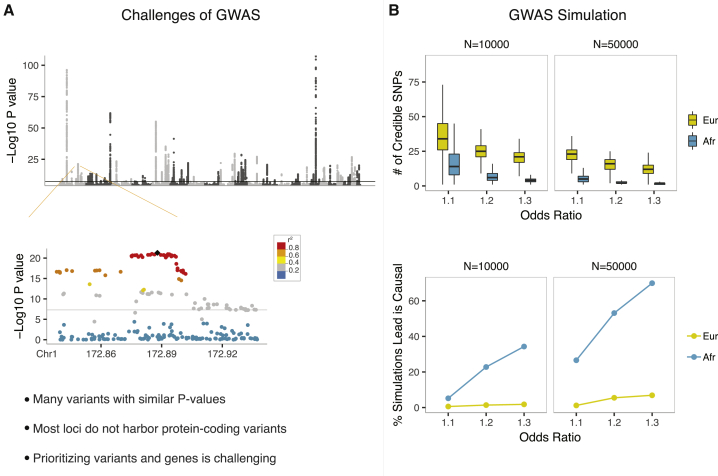
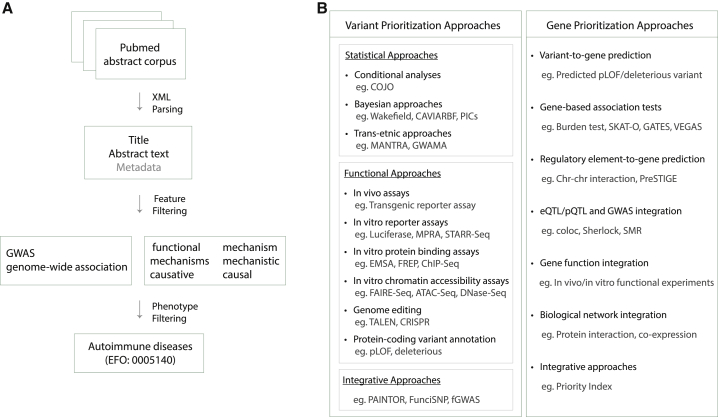
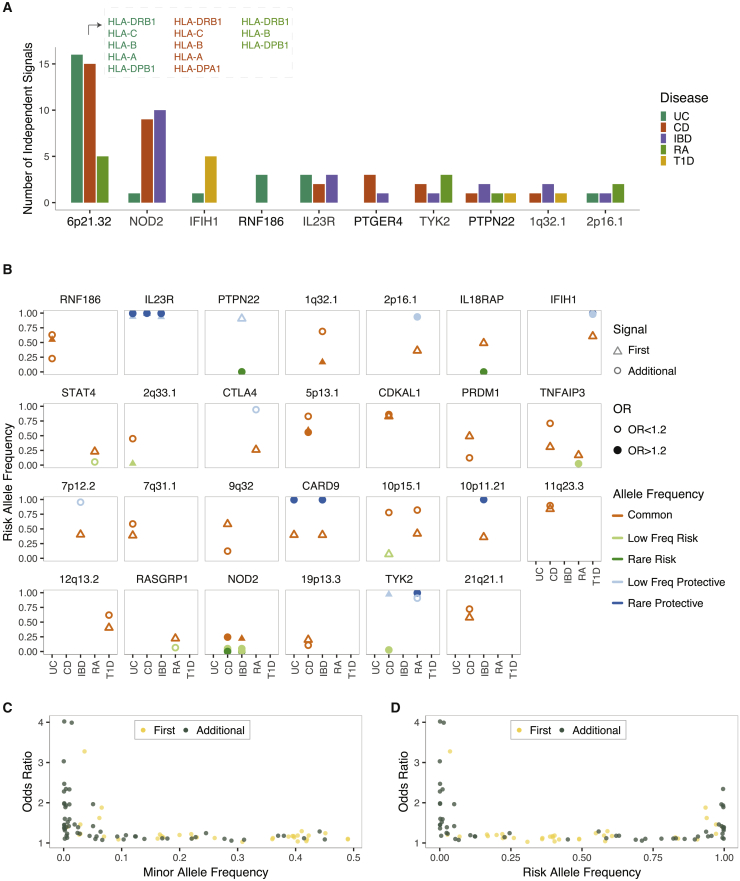
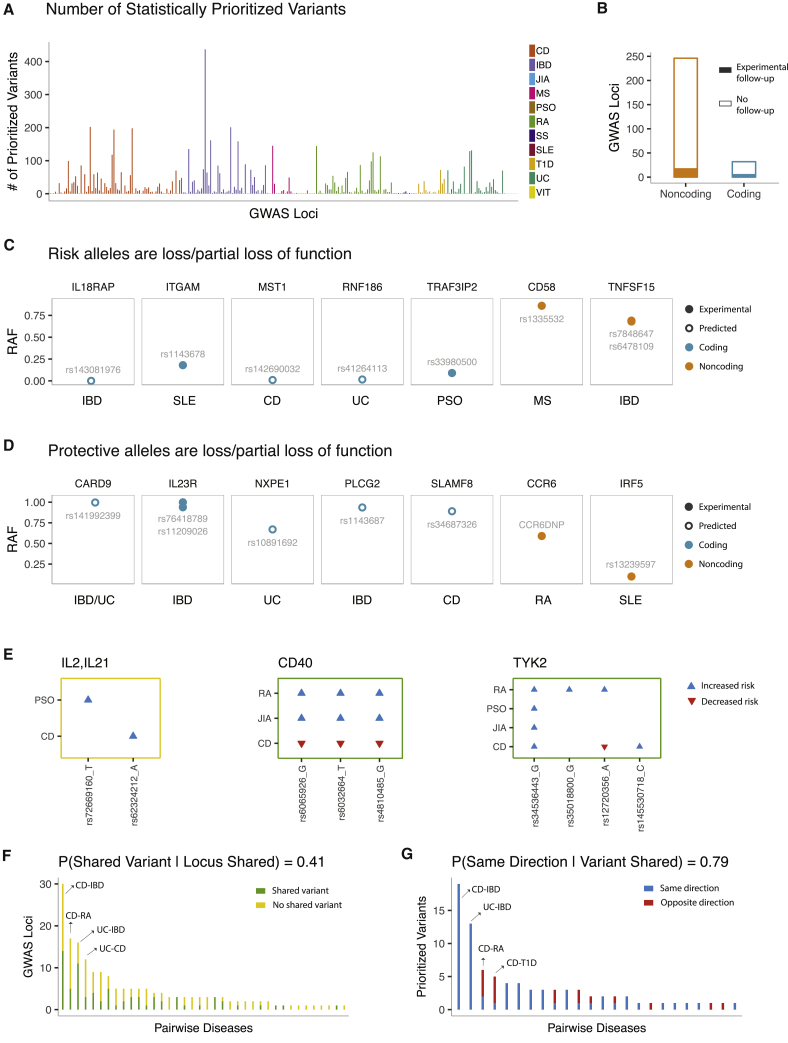
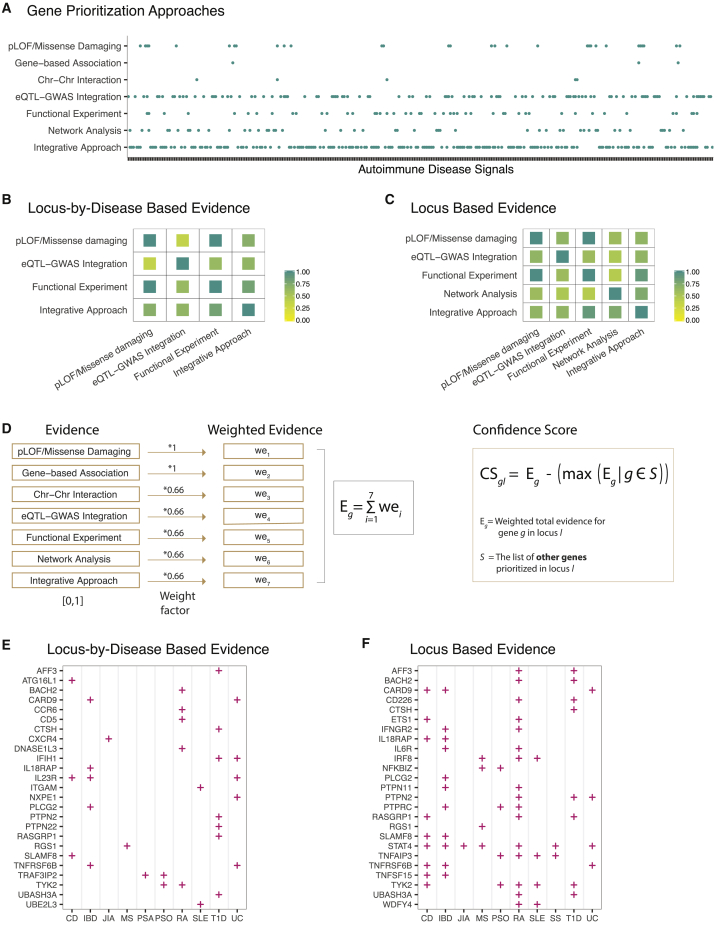
Genome-wide association studies (GWASs) have enabled unbiased identification of genetic loci contributing to common complex diseases. Because GWAS loci often harbor many variants and genes, it remains a major challenge to move from GWASs' statistical associations to the identification of causal variants and genes that underlie these association signals. Researchers have applied many statistical and functional fine-mapping strategies to prioritize genetic variants and genes as potential candidates. There is no gold standard in fine-mapping approaches, but consistent results across different approaches can improve confidence in the fine-mapping findings. Here, we combined text mining with a systematic review and formed a catalog of 85 studies with evidence of fine mapping for at least one autoimmune GWAS locus. Across all fine-mapping studies, we compiled 230 GWAS loci with allelic heterogeneity estimates and predictions of causal variants and trait-relevant genes. These 230 loci included 455 combinations of locus-by-disease association signals with 15 autoimmune diseases. Using these estimates, we assessed the probability of mediating disease risk associations across genes in GWAS loci and identified robust signals of causal disease biology. We predict that this comprehensive catalog of GWAS fine-mapping efforts in autoimmune disease will greatly help distill the plethora of information in the field and inform therapeutic strategies.
Copyright © 2021 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
M.C. is an employee of Bristol-Myers Squibb. J.C.M. is an employee and a shareholder of Bristol-Myers Squibb. C.D.B. declares no competing interests.
Figures
References
-
- Buniello A., MacArthur J.A.L., Cerezo M., Harris L.W., Hayhurst J., Malangone C., McMahon A., Morales J., Mountjoy E., Sollis E. The NHGRI-EBI GWAS Catalog of published genome-wide association studies, targeted arrays and summary statistics 2019. Nucleic Acids Res. 2019;47(D1):D1005–D1012. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
