

Determinants Associated With Longitudinal Adherence to Annual Lung Cancer Screening: A Retrospective Analysis of Claims Data
- PMID: 33798496
- PMCID: PMC8349785
- DOI: 10.1016/j.jacr.2021.03.003
Determinants Associated With Longitudinal Adherence to Annual Lung Cancer Screening: A Retrospective Analysis of Claims Data
Abstract
Objective: Lung cancer screening (LCS) efficacy is highly dependent on adherence to annual screening, but little is known about real-world adherence determinants. We used insurance claims data to examine associations between LCS annual adherence and demographic, comorbidity, health care usage, and geographic factors.
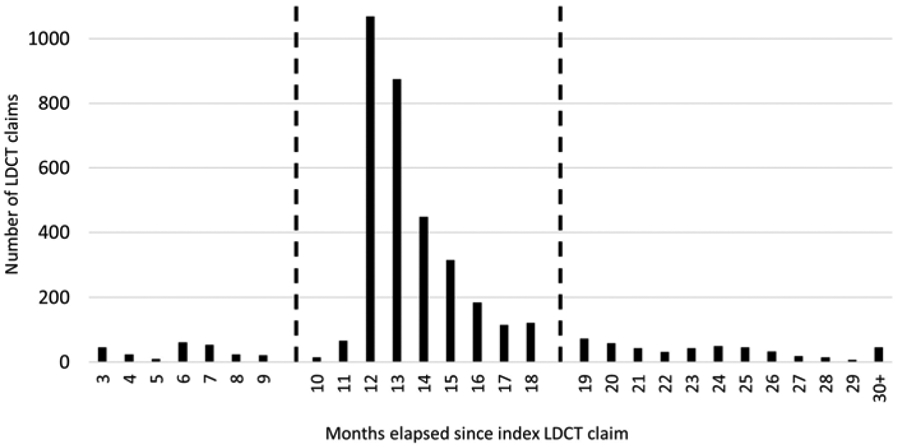
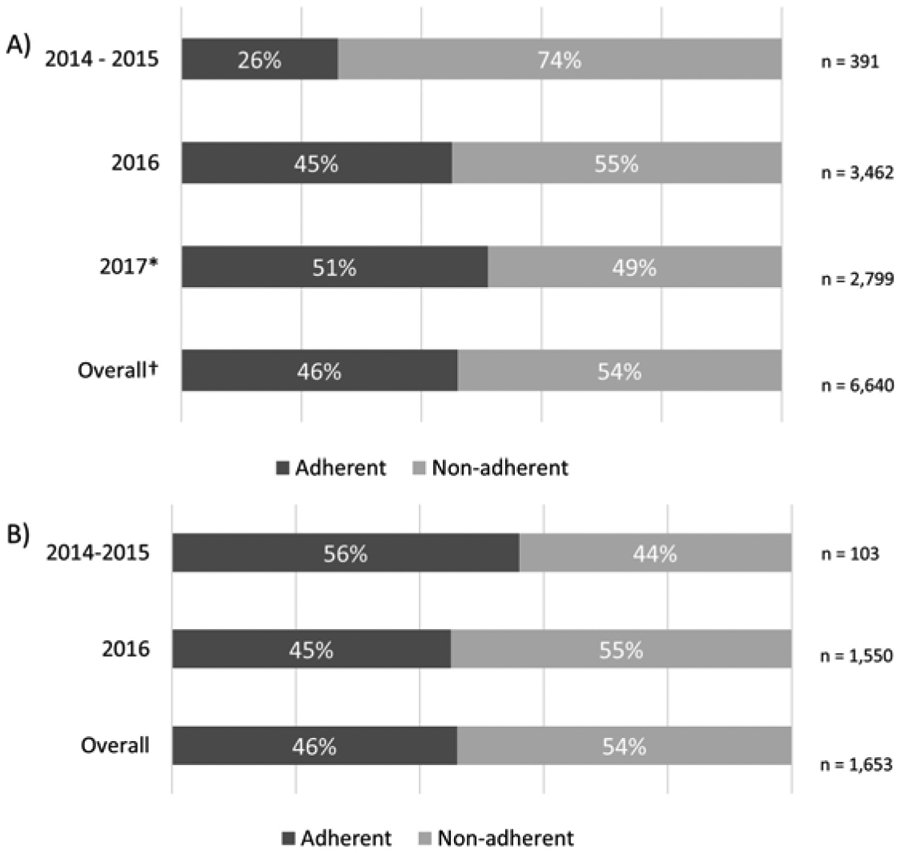
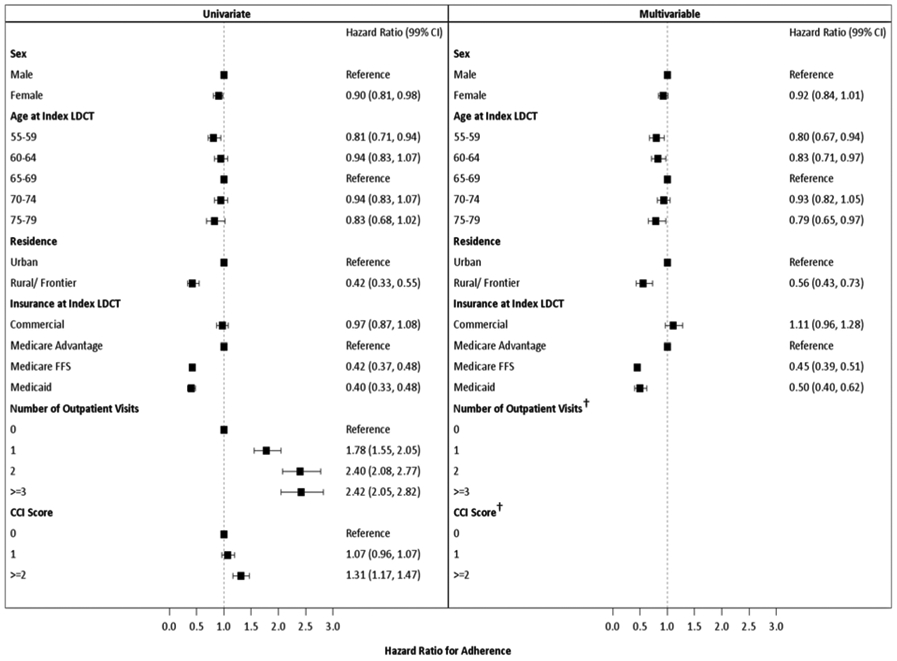
Materials and methods: Insurance claims data for all individuals with an LCS low-dose CT scan were obtained from the Colorado All Payer Claims Dataset. Adherence was defined as a second claim for a screening CT 10 to 18 months after the index claim. Cox proportional hazards regression was used to define the relationship between annual adherence and age, gender, insurance type, residence location, outpatient health care usage, and comorbidity burden.
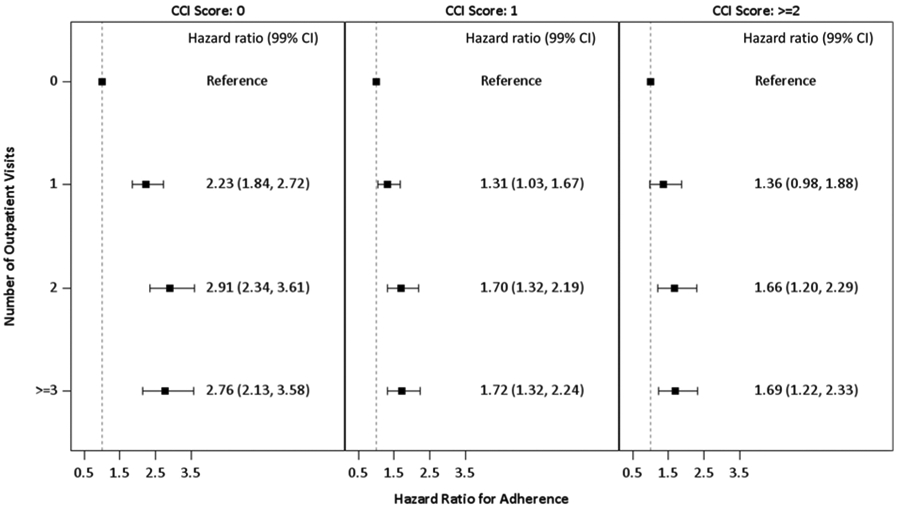
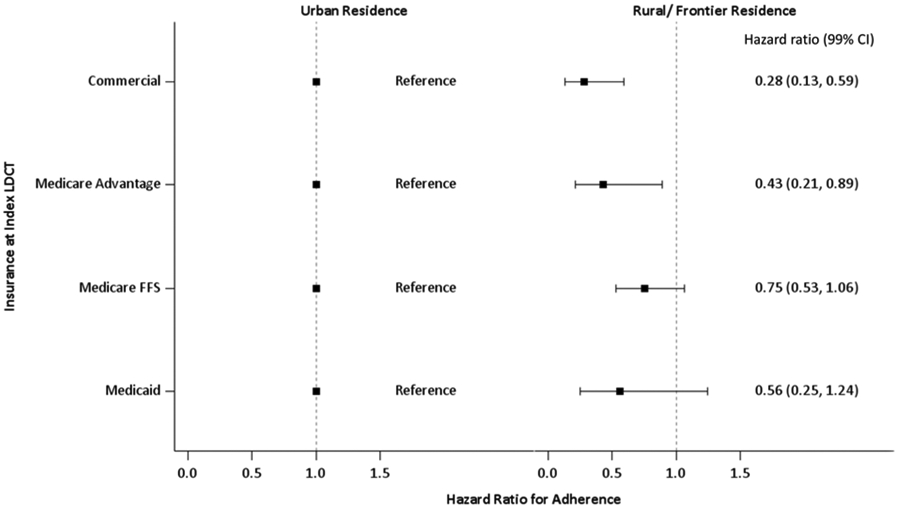
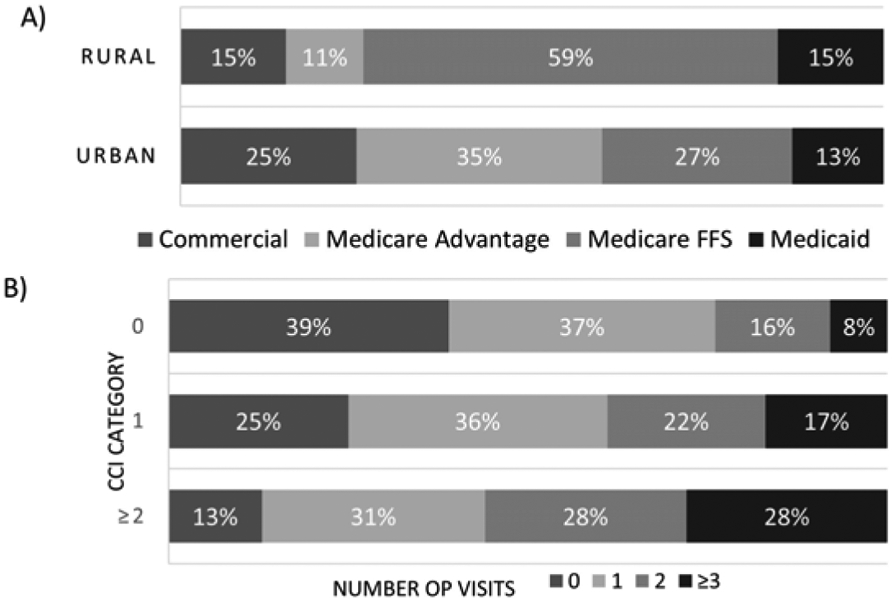
Results: After exclusions, the final data set consisted of 9,056 records with 3,072 adherent, 3,570 nonadherent, and 2,414 censored (unclassifiable) individuals. Less adherence was associated with ages 55 to 59 (hazard ratio [HR] = 0.80, 99% confidence interval [CI] = 0.67-0.94), 60 to 64 (HR = 0.83, 99% CI = 0.71-0.97), and 75 to 79 (HR = 0.79, 99% CI = 0.65-0.97); rural residence (HR = 0.56, 99% CI = 0.43-0.73); Medicare fee-for-service (HR = 0.45, 99% CI = 0.39-0.51), and Medicaid (HR = 0.50, 99% CI = 0.40-0.62). A significant interaction between outpatient health care usage and comorbidity was also observed. Increased outpatient usage was associated with increased adherence and was most pronounced for individuals without comorbidities.
Conclusions: This population-based description of LCS adherence determinants provides insight into populations that might benefit from specific interventions targeted toward improving adherence and maximizing LCS benefit. Quantifying population-based adherence rates and understanding factors associated with annual adherence are critical to improving screening adherence and reducing lung cancer death.
Keywords: Adherence determinants; cancer screening; lung cancer; patient adherence.
Copyright © 2021 American College of Radiology. All rights reserved.
Conflict of interest statement
Figures

Comment in
-
Lung Cancer Screening: A Necessary Tool Not Accessible for the Whole Population.J Am Coll Radiol. 2022 Mar;19(3):404. doi: 10.1016/j.jacr.2021.11.005. Epub 2022 Jan 7. J Am Coll Radiol. 2022. PMID: 35007508 No abstract available.
-
Authors' Response.J Am Coll Radiol. 2022 Mar;19(3):404-405. doi: 10.1016/j.jacr.2021.11.018. Epub 2022 Feb 8. J Am Coll Radiol. 2022. PMID: 35143785 No abstract available.
References
-
- American Cancer Society, Cancer Facts and Figures 2020. Available at: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-.... Accessed on June 11, 2020. - PMC - PubMed
-
- SEER cancer stat facts: lung and bronchus cancer. National Cancer Institute website. https://seer.cancer.gov/statfacts/html/lungb.html. Accessed on June 11, 2020.
-
- Koning HJ, van der Aalst CM, de Jong PA, et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N Engl J Med 2020; 382:503–513. - PubMed
-
- Centers for Medicare & Medicaid Services. Final National Coverage Determination on Screening for Lung Cancer with Low Dose Computed Tomography (LDCT). 2015. https://www.cms.gov/medicare-coverage-database/details/nca-decision-memo.... Accessed on June 11, 2020.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
