

A Cluster Randomized Trial to Reduce Missed Abusive Head Trauma in Pediatric Intensive Care Settings
- PMID: 33798512
- PMCID: PMC8403132
- DOI: 10.1016/j.jpeds.2021.03.055
A Cluster Randomized Trial to Reduce Missed Abusive Head Trauma in Pediatric Intensive Care Settings
Abstract
Objective: To estimate the impact of the PediBIRN (Pediatric Brain Injury Research Network) 4-variable clinical decision rule (CDR) on abuse evaluations and missed abusive head trauma in pediatric intensive care settings.
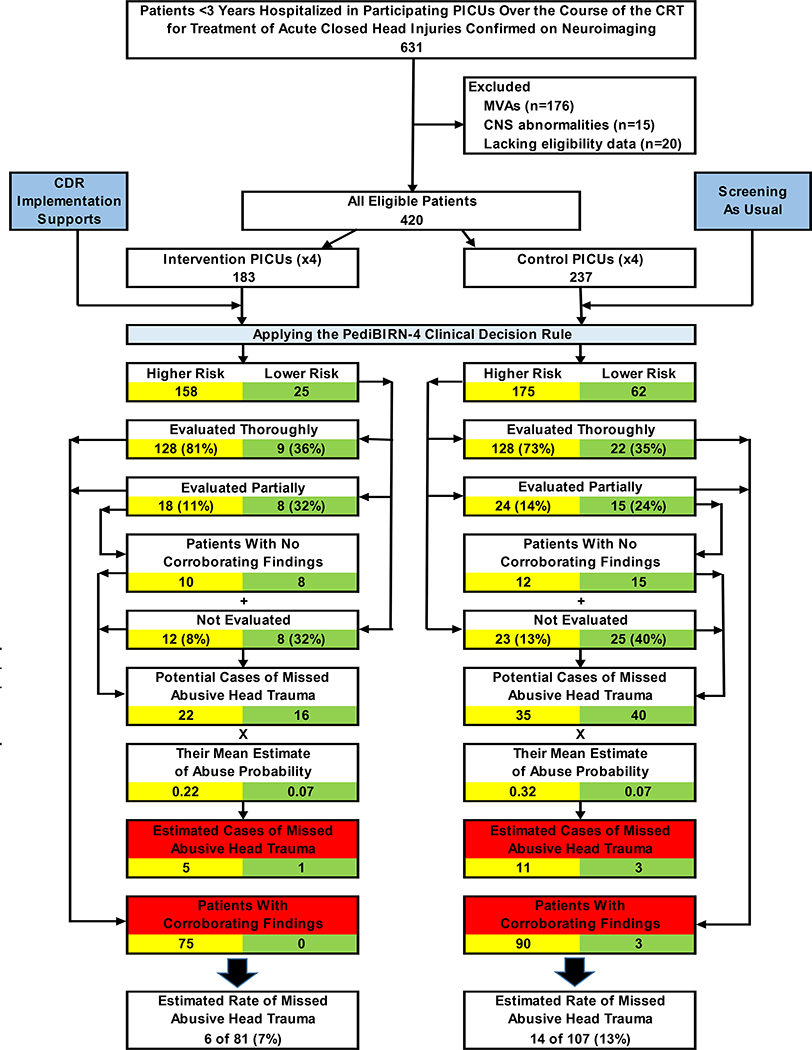
Study design: This was a cluster randomized trial. Participants included 8 pediatric intensive care units (PICUs) in US academic medical centers; PICU and child abuse physicians; and consecutive patients with acute head injures <3 years (n = 183 and n = 237, intervention vs control). PICUs were stratified by patient volumes, pair-matched, and randomized equally to intervention or control conditions. Randomization was concealed from the biostatistician. Physician-directed, cluster-level interventions included initial and booster training, access to an abusive head trauma probability calculator, and information sessions. Outcomes included "higher risk" patients evaluated thoroughly for abuse (with skeletal survey and retinal examination), potential cases of missed abusive head trauma (patients lacking either evaluation), and estimates of missed abusive head trauma (among potential cases). Group comparisons were performed using generalized linear mixed-effects models.
Results: Intervention physicians evaluated a greater proportion of higher risk patients thoroughly (81% vs 73%, P = .11) and had fewer potential cases of missed abusive head trauma (21% vs 32%, P = .05), although estimated cases of missed abusive head trauma did not differ (7% vs 13%, P = .22). From baseline (in previous studies) to trial, the change in higher risk patients evaluated thoroughly (67%→81% vs 78%→73%, P = .01), and potential cases of missed abusive head trauma (40%→21% vs 29%→32%, P = .003), diverged significantly. We did not identify a significant divergence in the number of estimated cases of missed abusive head trauma (15%→7% vs 11%→13%, P = .22).
Conclusions: PediBIRN-4 CDR application facilitated changes in abuse evaluations that reduced potential cases of missed abusive head trauma in PICU settings.
Trial registration: ClinicalTrials.gov: NCT03162354.
Keywords: child abuse; clinical decision rule; screening test.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures
Comment in
-
What Will it Take to Achieve Routine Screening for Abuse?J Pediatr. 2021 Sep;236:10-11. doi: 10.1016/j.jpeds.2021.05.038. Epub 2021 May 19. J Pediatr. 2021. PMID: 34022246 No abstract available.
-
Cluster Randomized Trials in Pediatric Research.J Pediatr. 2021 Sep;236:333-334. doi: 10.1016/j.jpeds.2021.06.008. Epub 2021 Jun 11. J Pediatr. 2021. PMID: 34126121 No abstract available.
Comment on
-
What Will it Take to Achieve Routine Screening for Abuse?J Pediatr. 2021 Sep;236:10-11. doi: 10.1016/j.jpeds.2021.05.038. Epub 2021 May 19. J Pediatr. 2021. PMID: 34022246 No abstract available.
References
-
- Duhaime AC, Christian CW, Rorke LB, Zimmerman RA. Nonaccidental head injury in infants--the “shaken-baby syndrome”. N Engl J Med 1998; 338:1822–9. - PubMed
-
- Keenan HT, Runyan DK, Marshall SW, Nocera MA, Merten DF, Sinal SH. A population-based study of inflicted traumatic brain injury in young children. JAMA 2003;290:621–6. - PubMed
-
- Eisele JA, Keglar SR, Trent RB, Coronado VG. Nonfatal traumatic brain injury-related hospitalization in very young children−−15 states. J Head Trauma Rehabil 2006;21:537–43. - PubMed
-
- Minns RA, Jones PA, Mok JY. Annual incidence of shaken impact syndrome in young children. Am J Prev Med 2008;34:S126–33. - PubMed
-
- Barlow KM, Minns RA. Annual incidence of shaken impact syndrome in young children. Lancet 2000;356:1571–2. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
