

Moderators of PTSD symptom change in group cognitive behavioral therapy and group present centered therapy
- PMID: 33799175
- PMCID: PMC8487250
- DOI: 10.1016/j.janxdis.2021.102386
Moderators of PTSD symptom change in group cognitive behavioral therapy and group present centered therapy
Abstract
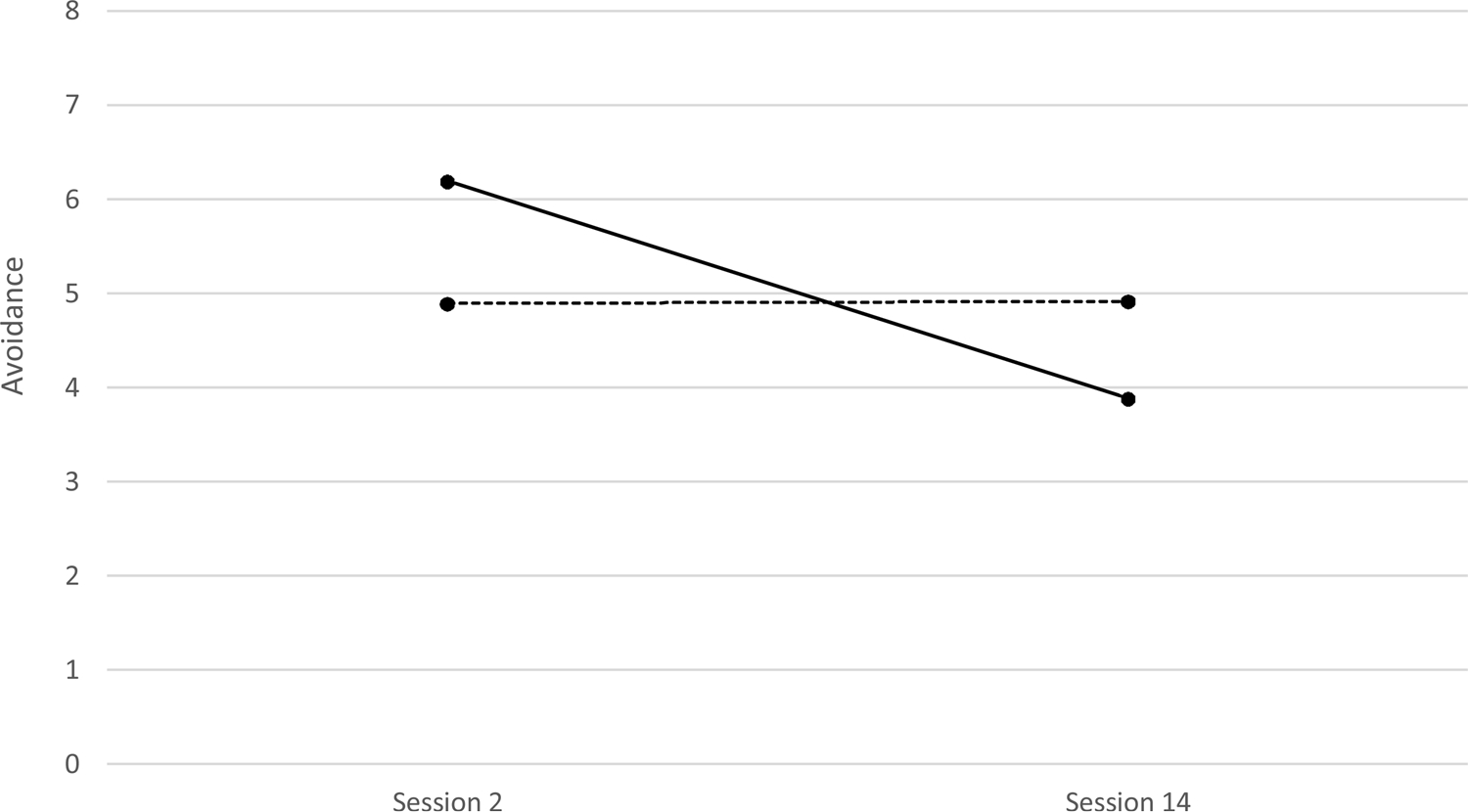
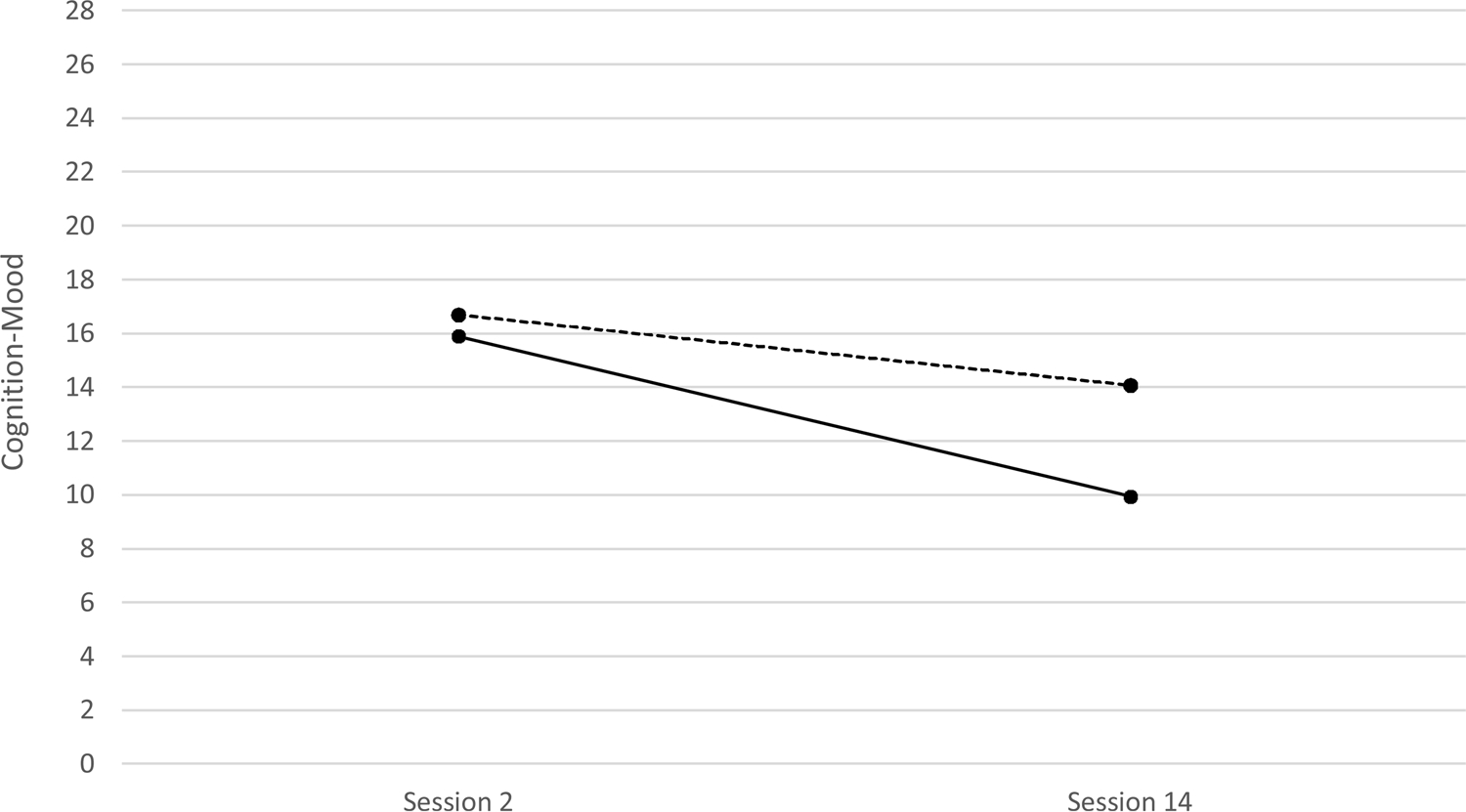
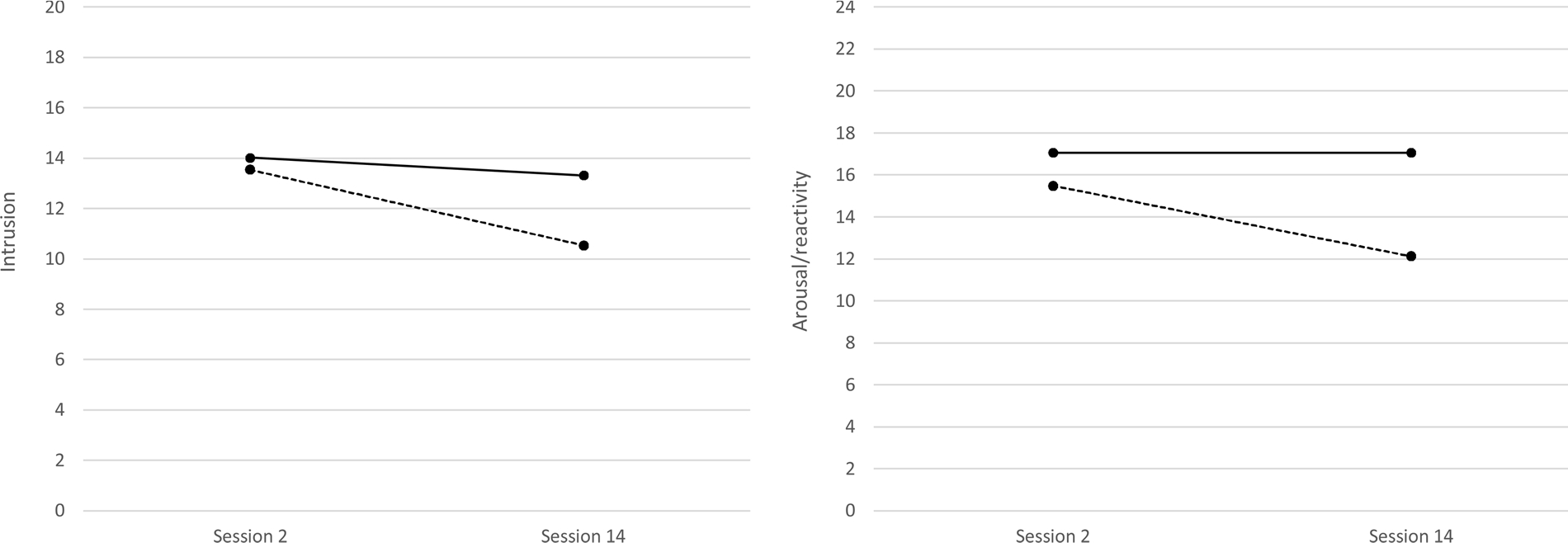
To examine moderators of change during group-based intervention for Posttraumatic Stress Disorder (PTSD), multilevel models were used to assess trajectories of symptom clusters in male veterans receiving trauma focused Group Cognitive Behavioral Treatment (gCBT; N = 84) or non-trauma focused Group Present Centered Therapy (gPCT; N = 91; Sloan et al., 2018). Separate models were conducted for symptom clusters in each intervention, examining pre-treatment PTSD symptoms, pre-treatment depression severity, age, index trauma, and outcome expectancies as potential moderators. Unconditioned growth models for both gCBT and gPCT showed reductions in intrusions, avoidance, negative cognitions/mood, and arousal/reactivity (all p < .001). Distinct moderators of recovery emerged for each treatment. Reductions in avoidance during gCBT were strongest at high levels of pre-treatment PTSD symptoms (low PTSD: p = .964, d = .05; high PTSD: p < .001, d = 1.31) whereas positive outcome expectancies enhanced reductions in cognitions/mood (low Expectancy: p = .120, d = .50; high Expectancy: p < .001, d = 1.13). For gPCT, high levels of pre-treatment depression symptoms negatively impacted change in both intrusion (low depression: p < .001, d = .96; high depression: p = .376, d = .22) and arousal/reactivity (low depression: p < .001, d = .95; high depression: p = .092, d = .39) symptoms. Results support the importance of examining trajectories of change and their moderators for specific treatments, particularly when contrasting trauma focused and non-trauma focused treatments.
Keywords: Moderator; PTSD; Treatment outcome; Veterans.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
A Randomized Controlled Trial of Group Cognitive Behavioral Treatment for Veterans Diagnosed With Chronic Posttraumatic Stress Disorder.J Trauma Stress. 2018 Dec;31(6):886-898. doi: 10.1002/jts.22338. Epub 2018 Nov 29. J Trauma Stress. 2018. PMID: 30499227 Free PMC article. Clinical Trial.
-
Cognitive-behavioral group treatment for veterans diagnosed with PTSD: Design of a hybrid efficacy-effectiveness clinical trial.Contemp Clin Trials. 2016 Mar;47:123-30. doi: 10.1016/j.cct.2015.12.016. Epub 2015 Dec 21. Contemp Clin Trials. 2016. PMID: 26718094 Free PMC article. Clinical Trial.
-
Examining changes in negative mood regulation expectancies, posttraumatic stress disorder, depression, and substance use following integrated cognitive-behavioral therapy.Subst Abus. 2017 Oct-Dec;38(4):468-472. doi: 10.1080/08897077.2017.1342736. Epub 2017 Jun 20. Subst Abus. 2017. PMID: 28632462 Clinical Trial.
-
Efficacy of group psychotherapy for posttraumatic stress disorder: Systematic review and meta-analysis of randomized controlled trials.Psychother Res. 2019 May;29(4):415-431. doi: 10.1080/10503307.2017.1405168. Epub 2017 Nov 27. Psychother Res. 2019. PMID: 29179647
-
Interventions for adults with a history of complex traumatic events: the INCiTE mixed-methods systematic review.Health Technol Assess. 2020 Sep;24(43):1-312. doi: 10.3310/hta24430. Health Technol Assess. 2020. PMID: 32924926 Free PMC article.
Cited by
-
Prognostic and prescriptive predictors of PTSD response to prolonged exposure and sertraline.J Mood Anxiety Disord. 2023 Jun 23;2:100008. doi: 10.1016/j.xjmad.2023.100008. eCollection 2023 Aug. J Mood Anxiety Disord. 2023. PMID: 40654373 Free PMC article.
-
Posttraumatic Stress Disorder Symptom Clusters in Surrogate Decision Makers of Patients Experiencing Chronic Critical Illness.Crit Care Explor. 2022 Mar 1;4(3):e0647. doi: 10.1097/CCE.0000000000000647. eCollection 2022 Mar. Crit Care Explor. 2022. PMID: 35261980 Free PMC article.
References
-
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: American Psychiatric Association.
-
- American Psychological Association Guideline Development Panel for the Treatment of PTSD. (2017). Summary of recommendations. https://www.apa.org/ptsdguideline/treatments/recommendations-summary-tab....
-
- Beck JG and Sloan DM (2021) Group treatments for PTSD. In Friedman MJ, Keane TM, and Schnurr P (Eds). Handbook of PTSD: Science & Practice (3rd ed.). New York: Guilford Press. In press.
-
- Beck AT, Steer RA, & Brown GK (1996). Manual for beck depression inventory-II. San Antonio, TX: Psychological Corporation.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
