

Transitioning the Molecular Tumor Board from Proof of Concept to Clinical Routine: A German Single-Center Analysis
- PMID: 33800365
- PMCID: PMC7962829
- DOI: 10.3390/cancers13051151
Transitioning the Molecular Tumor Board from Proof of Concept to Clinical Routine: A German Single-Center Analysis
Abstract
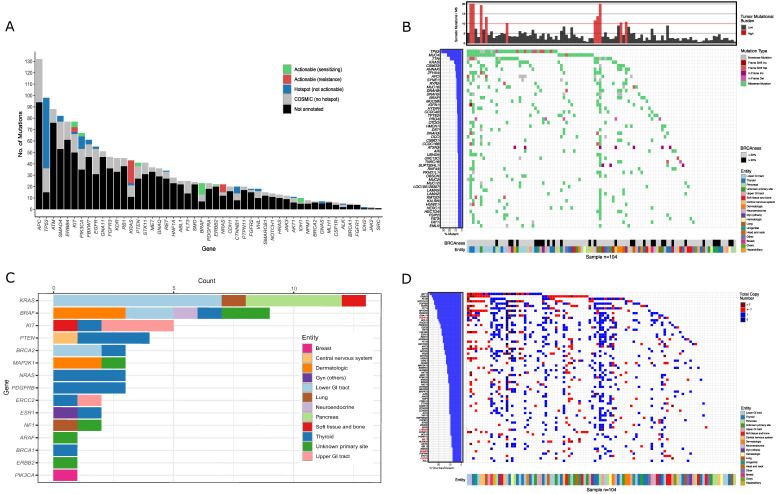
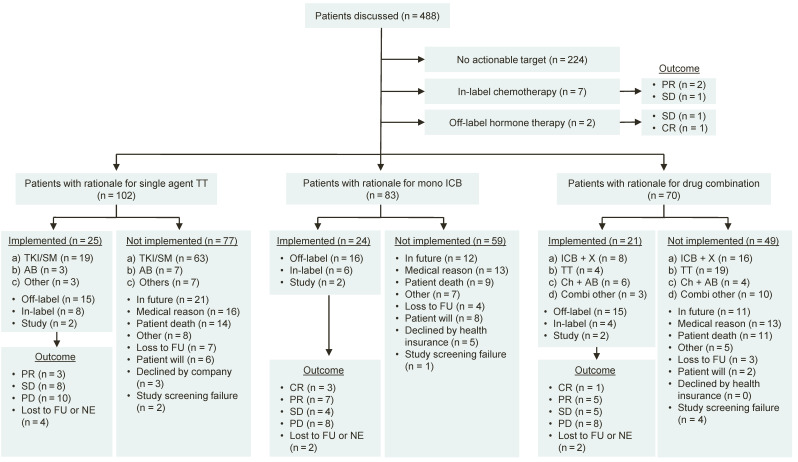
Molecular precision oncology faces two major challenges: first, to identify relevant and actionable molecular variants in a rapidly changing field and second, to provide access to a broad patient population. Here, we report a four-year experience of the Molecular Tumor Board (MTB) of the Comprehensive Cancer Center Freiburg (Germany) including workflows and process optimizations. This retrospective single-center study includes data on 488 patients enrolled in the MTB from February 2015 through December 2018. Recommendations include individual molecular diagnostics, molecular stratified therapies, assessment of treatment adherence and patient outcomes including overall survival. The majority of MTB patients presented with stage IV oncologic malignancies (90.6%) and underwent an average of 2.1 previous lines of therapy. Individual diagnostic recommendations were given to 487 patients (99.8%). A treatment recommendation was given in 264 of all cases (54.1%) which included a molecularly matched treatment in 212 patients (43.4%). The 264 treatment recommendations were implemented in 76 patients (28.8%). Stable disease was observed in 19 patients (25.0%), 17 had partial response (22.4%) and five showed a complete remission (6.6%). An objective response was achieved in 28.9% of cases with implemented recommendations and for 4.5% of the total population (22 of 488 patients). By optimizing the MTB workflow, case-discussions per session increased significantly while treatment adherence and outcome remained stable over time. Our data demonstrate the feasibility and effectiveness of molecular-guided personalized therapy for cancer patients in a clinical routine setting showing a low but robust and durable disease control rate over time.
Keywords: cancer genetics; cancer immunotherapy; cancer molecular biology; cancer progression; combination therapies; molecular profiling; molecular tumor board; personalized cancer medicine; precision oncology; targeted therapies.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Mullard A. NEWS & AnaLYSIS 2018 FDA Drug Approvals. Nat. Rev. Drug Discov. 2019;18:85–89. - PubMed
-
- U.S. Food and Drug Administration (FDA) Grants Accelerated Approval to Pembrolizumab for First Tissue/Site Agnostic Indication. FDA; Rockwell, MD, USA: 2017.
-
- U.S. Food and Drug Administration (FDA) Approves Pembrolizumab for the First-Line Treatment of MSI-H/DMMR Colorectal Cancer. [(accessed on 10 January 2021)]; Available online: https://www.ascopost.com/issues/july-10-2020/fda-approves-pembrolizumab-...
-
- U.S. Food and Drug Administration (FDA) Approves Pembrolizumab for Adults and Children with TMB-H Solid Tumors. [(accessed on 10 January 2021)]; Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-pemb....
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
