

Combination Assessment of Diffusion-Weighted Imaging and T2-Weighted Imaging Is Acceptable for the Differential Diagnosis of Lung Cancer from Benign Pulmonary Nodules and Masses
- PMID: 33800560
- PMCID: PMC8037373
- DOI: 10.3390/cancers13071551
Combination Assessment of Diffusion-Weighted Imaging and T2-Weighted Imaging Is Acceptable for the Differential Diagnosis of Lung Cancer from Benign Pulmonary Nodules and Masses
Abstract
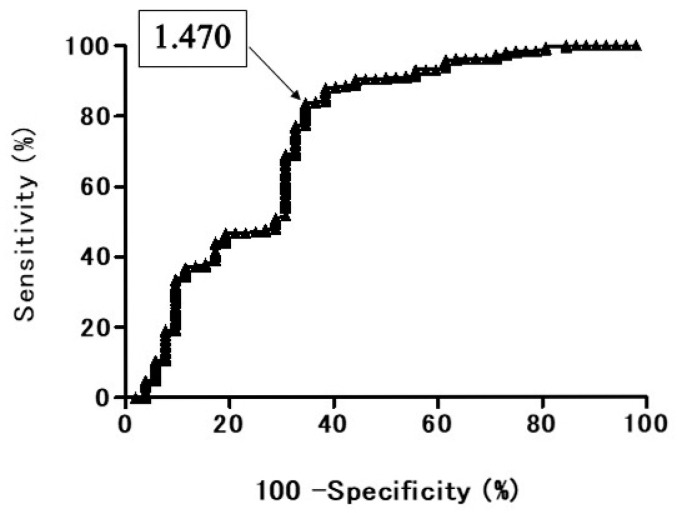
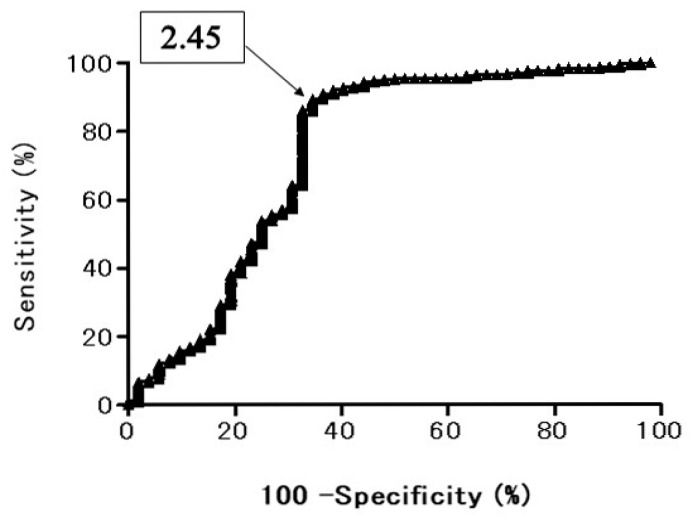
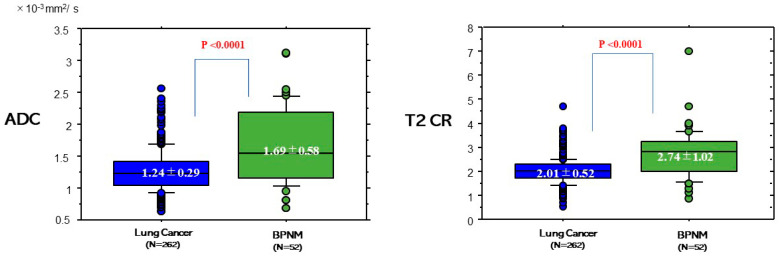
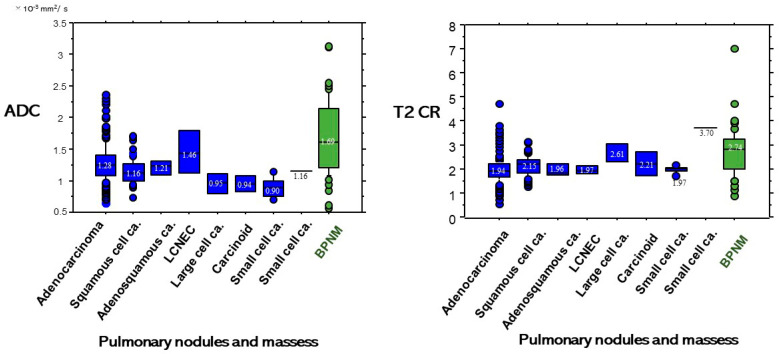
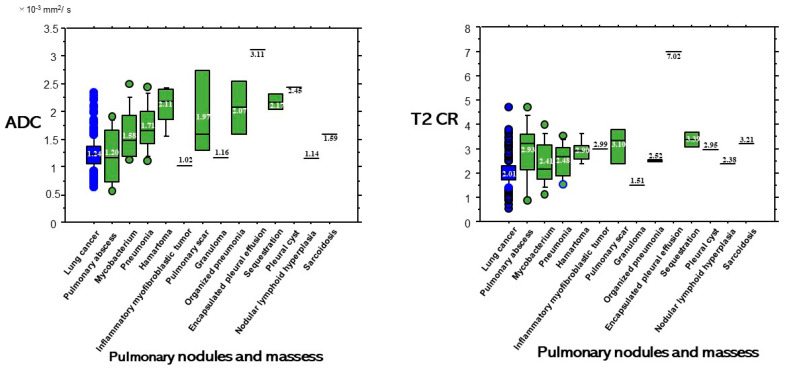
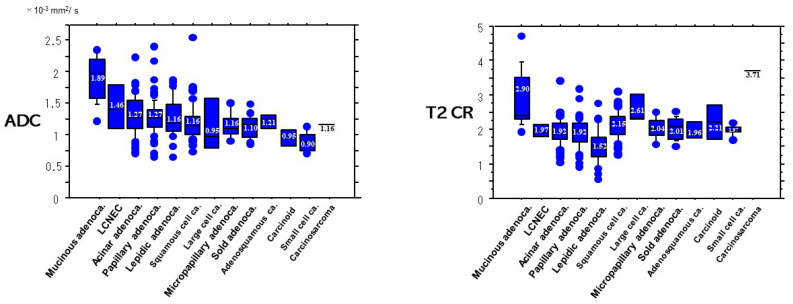
The purpose of this study is to determine whether the combination assessment of DWI and T2-weighted imaging (T2WI) improves the diagnostic ability for differential diagnosis of lung cancer from benign pulmonary nodules and masses (BPNMs). The optimal cut-off value (OCV) for differential diagnosis was set at 1.470 × 10-3 mm2/s for apparent diffusion coefficient (ADC), and at 2.45 for T2 contrast ratio (T2 CR). The ADC (1.24 ± 0.29 × 10-3 mm2/s) of lung cancer was significantly lower than that (1.69 ± 0.58 × 10-3 mm2/s) of BPNM. The T2 CR (2.01 ± 0.52) of lung cancer was significantly lower than that (2.74 ± 1.02) of BPNM. As using the OCV for ADC, the sensitivity was 83.9% (220/262), the specificity 63.4% (33/52), and the accuracy 80.6% (253/314). As using the OCV for T2 CR, the sensitivity was 89.7% (235/262), the specificity 61.5% (32/52), and the accuracy 85.0% (267/314). In 212 PNMs which were judged to be malignant by both DWI and T2WI, 203 PNMs (95.8%) were lung cancers. In 33 PNMs which were judged to be benign by both DWI and T2WI, 23 PNMs (69.7%) were BPNMs. The combined assessment of DWI and T2WI could judge PNMs more precisely and would be acceptable for differential diagnosis of PNMs.
Keywords: T2-weighted imaging (T2WI); apparent diffusion coefficient (ADC); diffusion-weighted magnetic resonance imaging (DWI); lung cancer; magnetic resonance imaging (MRI); pulmonary abscess; pulmonary nodule and mass (PNM).
Conflict of interest statement
All authors have no conflict of interest to declare.
Figures
References
-
- Could M.K., Maclean C.C., Kuschner W.G., Rydzak C.E., Owens D.K. Accuracy of positron emission tomography for diagnosis of pulmonary nodules and mass lesions: A meta-analysis. JAMA. 2001;285:914–924. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
